Recommendations
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
12<br />
Smith et al. 2005<br />
ACC/AHA/SCAI Practice Guidelines<br />
ACC - www.acc.org<br />
AHA - www.americanheart.org<br />
SCAI - www.scai.org<br />
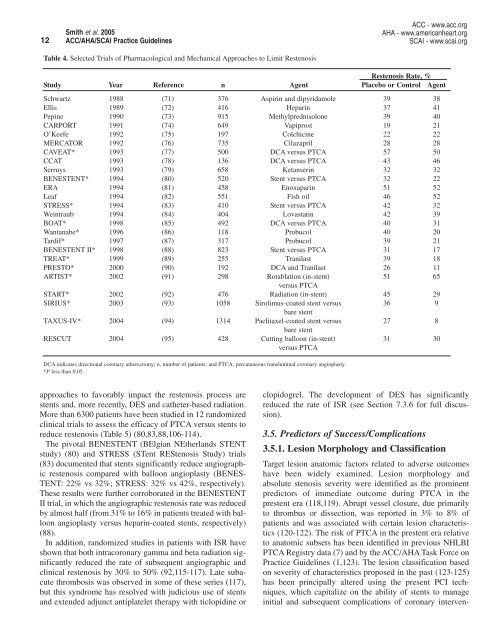
Table 4. Selected Trials of Pharmacological and Mechanical Approaches to Limit Restenosis<br />
Restenosis Rate, %<br />
Study Year Reference n Agent Placebo or Control Agent<br />
Schwartz 1988 (71) 376 Aspirin and dipyridamole 39 38<br />
Ellis 1989 (72) 416 Heparin 37 41<br />
Pepine 1990 (73) 915 Methylprednisolone 39 40<br />
CARPORT 1991 (74) 649 Vapiprost 19 21<br />
O’Keefe 1992 (75) 197 Colchicine 22 22<br />
MERCATOR 1992 (76) 735 Cilazapril 28 28<br />
CAVEAT* 1993 (77) 500 DCA versus PTCA 57 50<br />
CCAT 1993 (78) 136 DCA versus PTCA 43 46<br />
Serruys 1993 (79) 658 Ketanserin 32 32<br />
BENESTENT* 1994 (80) 520 Stent versus PTCA 32 22<br />
ERA 1994 (81) 458 Enoxaparin 51 52<br />
Leaf 1994 (82) 551 Fish oil 46 52<br />
STRESS* 1994 (83) 410 Stent versus PTCA 42 32<br />
Weintraub 1994 (84) 404 Lovastatin 42 39<br />
BOAT* 1998 (85) 492 DCA versus PTCA 40 31<br />
Wantanabe* 1996 (86) 118 Probucol 40 20<br />
Tardif* 1997 (87) 317 Probucol 39 21<br />
BENESTENT II* 1998 (88) 823 Stent versus PTCA 31 17<br />
TREAT* 1999 (89) 255 Tranilast 39 18<br />
PRESTO* 2000 (90) 192 DCA and Tranilast 26 11<br />
ARTIST* 2002 (91) 298 Rotablation (in-stent) 51 65<br />
versus PTCA<br />
START* 2002 (92) 476 Radiation (in-stent) 45 29<br />
SIRIUS* 2003 (93) 1058 Sirolimus-coated stent versus 36 9<br />
bare stent<br />
TAXUS-IV* 2004 (94) 1314 Paclitaxel-coated stent versus 27 8<br />
bare stent<br />
RESCUT 2004 (95) 428 Cutting balloon (in-stent) 31 30<br />
versus PTCA<br />
DCA indicates directional coronary atherectomy; n, number of patients; and PTCA, percutaneous transluminal coronary angioplasty.<br />
*P less than 0.05.<br />
approaches to favorably impact the restenosis process are<br />
stents and, more recently, DES and catheter-based radiation.<br />
More than 6300 patients have been studied in 12 randomized<br />
clinical trials to assess the efficacy of PTCA versus stents to<br />
reduce restenosis (Table 5) (80,83,88,106-114).<br />
The pivotal BENESTENT (BElgian NEtherlands STENT<br />
study) (80) and STRESS (STent REStenosis Study) trials<br />
(83) documented that stents significantly reduce angiographic<br />
restenosis compared with balloon angioplasty (BENES-<br />
TENT: 22% vs 32%; STRESS: 32% vs 42%, respectively).<br />
These results were further corroborated in the BENESTENT<br />
II trial, in which the angiographic restenosis rate was reduced<br />
by almost half (from 31% to 16% in patients treated with balloon<br />
angioplasty versus heparin-coated stents, respectively)<br />
(88).<br />
In addition, randomized studies in patients with ISR have<br />
shown that both intracoronary gamma and beta radiation significantly<br />
reduced the rate of subsequent angiographic and<br />
clinical restenosis by 30% to 50% (92,115-117). Late subacute<br />
thrombosis was observed in some of these series (117),<br />
but this syndrome has resolved with judicious use of stents<br />
and extended adjunct antiplatelet therapy with ticlopidine or<br />
clopidogrel. The development of DES has significantly<br />
reduced the rate of ISR (see Section 7.3.6 for full discussion).<br />
3.5. Predictors of Success/Complications<br />
3.5.1. Lesion Morphology and Classification<br />
Target lesion anatomic factors related to adverse outcomes<br />
have been widely examined. Lesion morphology and<br />
absolute stenosis severity were identified as the prominent<br />
predictors of immediate outcome during PTCA in the<br />
prestent era (118,119). Abrupt vessel closure, due primarily<br />
to thrombus or dissection, was reported in 3% to 8% of<br />
patients and was associated with certain lesion characteristics<br />
(120-122). The risk of PTCA in the prestent era relative<br />
to anatomic subsets has been identified in previous NHLBI<br />
PTCA Registry data (7) and by the ACC/AHA Task Force on<br />
Practice Guidelines (1,123). The lesion classification based<br />
on severity of characteristics proposed in the past (123-125)<br />
has been principally altered using the present PCI techniques,<br />
which capitalize on the ability of stents to manage<br />
initial and subsequent complications of coronary interven-