Recommendations
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
16<br />
Smith et al. 2005<br />
ACC/AHA/SCAI Practice Guidelines<br />
ACC - www.acc.org<br />
AHA - www.americanheart.org<br />
SCAI - www.scai.org<br />
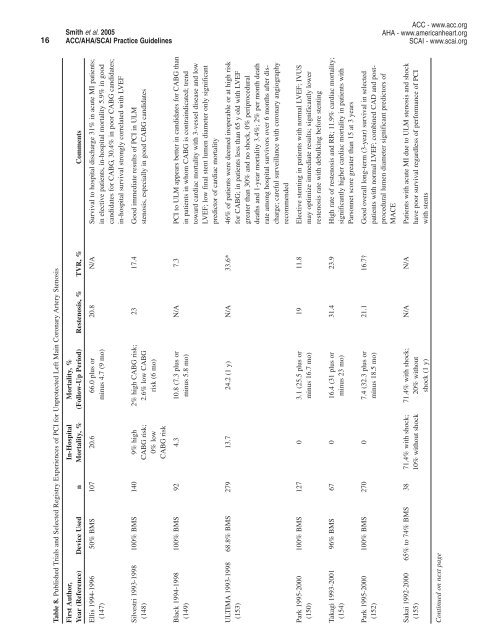
Table 8. Published Trials and Selected Registry Experiences of PCI for Unprotected Left Main Coronary Artery Stenosis<br />
First Author, In-Hospital Mortality, %<br />
Year (Reference) Device Used n Mortality, % (Follow-Up Period) Restenosis, % TVR, % Comments<br />
Ellis 1994-1996 50% BMS 107 20.6 66.0 plus or 20.8 N/A Survival to hospital discharge 31% in acute MI patients;<br />
(147) minus 4.7 (9 mo) in elective patients, in-hospital mortality 5.9% in good<br />
candidates for CABG, 30.4% in poor CABG candidates;<br />
in-hospital survival strongly correlated with LVEF<br />
Silvestri 1993-1998 100% BMS 140 9% high 2% high CABG risk; 23 17.4 Good immediate results of PCI in ULM<br />
(148) CABG risk; 2.6% low CABG stenosis, especially in good CABG candidates<br />
0% low risk (6 mo)<br />
CABG risk<br />
Black 1994-1998 100% BMS 92 4.3 10.8 (7.3 plus or N/A 7.3 PCI to ULM appears better in candidates for CABG than<br />
(149) minus 5.8 mo) in patients in whom CABG is contraindicated; trend<br />
toward cardiac mortality with 3-vessel disease and low<br />
LVEF; low final stent lumen diameter only significant<br />
predictor of cardiac mortality<br />
ULTIMA 1993-1998 68.8% BMS 279 13.7 24.2 (1 y) N/A 33.6* 46% of patients were deemed inoperable or at high risk<br />
(153) for CABG; in patients less than 65 y old with LVEF<br />
greater than 30% and no shock, 0% periprocedural<br />
deaths and 1-year mortality 3.4%; 2% per month death<br />
rate among hospital survivors over 6 months after discharge;<br />
careful surveillance with coronary angiography<br />
recommended<br />
Park 1995-2000 100% BMS 127 0 3.1 (25.5 plus or 19 11.8 Elective stenting in patients with normal LVEF; IVUS<br />
(150) minus 16.7 mo) may optimize immediate results; significantly lower<br />
restenosis rate with debulking before stenting<br />
Takagi 1993-2001 96% BMS 67 0 16.4 (31 plus or 31.4 23.9 High rate of restenosis and RR; 11.9% cardiac mortality;<br />
(154) minus 23 mo) significantly higher cardiac mortality in patients with<br />
Parsonnet score greater than 15 at 3 years<br />
Park 1995-2000 100% BMS 270 0 7.4 (32.3 plus or 21.1 16.7† Good overall long-term (3-year) survival in selected<br />
(152) minus 18.5 mo) patients with normal LVEF; combined CAD and postprocedural<br />
lumen diameter significant predictors of<br />
MACE<br />
Sakai 1992-2000 65% to 74% BMS 38 71.4% with shock; 71.4% with shock; N/A N/A Patients with acute MI due to ULM stenosis and shock<br />
(155) 10% without shock 20% without have poor survival regardless of performance of PCI<br />
shock (1 y) with stents<br />
Continued on next page