Recommendations
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
ACC/AHA/SCAI PCI Guidelines - British Cardiovascular Intervention ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
48<br />
Smith et al. 2005<br />
ACC/AHA/SCAI Practice Guidelines<br />
ACC - www.acc.org<br />
AHA - www.americanheart.org<br />
SCAI - www.scai.org<br />
(378)<br />
(415)<br />
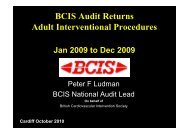
Figure 8. Comparison of elapsed time to fibrinolysis versus primary PCI. Time is presented as a continuous variable in minutes on<br />
the horizontal axis. For DANAMI-2, times reflect components of delay from symptom onset to randomization (vertical bar) and are<br />
further separated according to whether patients presented at community referral hospitals or those equipped for primary PCI. For<br />
those patients randomized to PCI at a referral hospital, the 3 components of delay after randomization are related to duration of stay<br />
at referral hospital, time for transport to PCI hospital, and delay from arrival at PCI hospital to balloon inflation. Lysis indicates fibrinolysis;<br />
PCI, percutaneous coronary intervention; Rand, randomization; SK, streptokinase; and Transp, transportation. Top graph<br />
reprinted with permission from Anderson et al. N Engl J Med 2003;349:733-42 (378). Copyright 2003 Massachusetts Medical Society.<br />
All rights reserved. Bottom graph reprinted from Widimsky et al. Eur Heart J 2003;24:94-104 (415) with permission from the<br />
European Society of Cardiology.<br />
33% relative risk reduction with primary PCI compared with<br />
a 9% relative risk reduction with fibrinolytic therapy (447-<br />
449). Primary PCI in patients with anterior STEMI reduces<br />
mortality compared with fibrinolytic therapy, but there is no<br />
difference in patients with nonanterior STEMI (450,451).<br />
Despite the evidence supporting primary PCI in the treatment<br />
of STEMI, there is serious concern that a routine policy<br />
of primary PCI for patients with STEMI will result in<br />
unacceptable delays in achieving reperfusion in a substantial<br />
number of patients and less than optimal outcomes if performed<br />
by less experienced operators. The mean time delay<br />
for PCI instead of fibrinolysis in the randomized trials was<br />
only 40 min (364). Strict performance criteria must be mandated<br />
for primary angioplasty programs so that excessive<br />
delays in reperfusion and performance by low-volume or<br />
poor-outcome operators/centers do not occur. The physicians,<br />
nursing, and technical catheterization laboratory staff<br />
must be experienced in handling acutely ill patients, must be<br />
skilled in all aspects of interventional equipment and procedures,<br />
and must participate in a 24-hours-per-day, 365-daysper-year<br />
call schedule. Interventional cardiologists and centers<br />
should strive for 1) balloon dilation within 90 min of<br />
admission and diagnosis of STEMI (452); 2) TIMI 2 to 3<br />
flow attained in more than 90% of patients; 3) emergency<br />
CABG rate less than 2% among all patients undergoing the<br />
procedure; 4) actual performance of PCI in 85% of patients<br />
brought to the laboratory; and 5) a risk-adjusted in-hospital<br />
mortality rate less than 7% in patients without cardiogenic