■ Primaire posttraumatische amputatie, wanneer te verrichten en welk niveau te kiezen?V o l18dec’11Literatuur1. Prevention of infection in the treatment of one thousandand twenty-five open fractures of long bones: retrospectiveand prospective analyses. Gustilo RB, Anderson JT. J BoneJoint Surg Am. 1976;58:453-4582. Problems in the management of type III (severe) openfractures: A new classification of type III open fractures.Gustilo RB, Mendoza RM, Williams DN. J Trauma.1984;24:742-63. A new classification of soft-tissue damage in open andclosed fractures. Tscherne H, Oestern HJ. Unfallheilkunde.1982;85:111-54. Objective criteria accurately predict amputation followinglower extremity injury. K Johansen, M Daines, T Howey, DHelfet, ST Hansen. JOT 19905. Limb salvage vs amputation; premliminary results of hetMangled Extremity Severity Score. DL Helfet, T Howey, RSanders, K Johanssen. Clinical orthopaedics and relatedresearch. July 1990.6. The type III-C tibial fracture. Salvage or amputation. STHansen. J Bone Joint Surg Am. 1987;69:799-8007. Salvage of lower extremities following combined orthopaedicand vascular trauma. A predictive salvage score. HoweHR, Poole GV, Hansen KJ, Clark T, Plonk GW, Koman LA,Pennell TC. Am Surg. 1987;53:205-2088. Severe open fracture of the lower extremity: a retrospectiveevaluation of the Mangled Extremity Severity Score.Mc Namara MG, Heckman JD, Corley EG. J Orthop Trauma.1994;213:473-819. The futility of predictive scoring of mangled lower extremities.Bonanni F, Rhodes M, Lucke JF. J Trauma. 1993;34:99-10410. Limb reconstruction versus amputation decision making inmassive lower extremity trauma. Lange RH. Clin Orthop.1989;243:92-911. Lower Extremity Assessment Project (LEAP)-The bestavailable evidence on limb-threatening lower extremitytrauma. TF Higgins, JB Klatt, TC Beals. Orthop Clin N Am 41(2010) 233-239.12. A prospective evaluation of the clinical utility of the lowerextremityinjury severity scores. MJ Bosse, EJ MacKenzie, JFKellam, AR Burgess, LX Webb, MF Swiontkowski, RW Sanders,AL Jones, MP McAndrew, BM Patterson, ML McCarthy, JKCyril. J Bone Joint Surg Am 2001;83:313. Salvage after severe lower-extremity trauma: Are theoutcomes worth the means? AB Dagum, K Andrew, EHSchemitsch, JL Mahoney, MN Mahomed, KR Blight. Plasticand reconstructive surgery. April 199914. Ability of lower-extremity injury severity scores to predictfunctional outcome after limb salvage. Ly TV, Travison, TG,Castillo RC, Bosse MJ, Mackenzie EJ and the LEAP studygroup. J Bone Joint Surg Am. 2008;90:1783-174315. The insensate foot following severe lower extremity trauma.An indication for amputation? MJ Bosse, ML McCarthy, ALJones, LX Webb, SH Sims, RW Sanders, AJ McKenzie and theLEAP study group. J Bone Joint Surg AM 2005;87:2601-260816. A philosophy of care of op open injuries based on the Gangahospital score. Rajasekaran S, Raja Sabapathy S. Injury2007;38:137-14617. The utility of scores in the decision to salvage or amputationin severely injured limbs. Rajasekaran S. Indian JOrthop. 2008;42(4):368-37618. A score for predicting salvage and outcome in Gustilo typeIII-A and type III-B open tibial fractures. Rajasekaran S,Naresh Babu J, Dheenadhayalan J, et al. J Bone Joint SurgBr 2006;88-B:1351-6019. Level of lower limb amputation in relation to etiology; anepidemiological study. Ebskov LB. Prosth & Orthot Int, 16:163-167 1992.20. Amputatie en prothesiologie van de onderste extemiteit.JHB Geertzen, JS Rietman. Lemma BV Utrecht2002. Hoofdstuk 3 Amputatieniveaus. 57-68 Hoofdstuk 6Amputaties bij ongevalspatienten. 95-10821. Report of ISPO concencus conference on amputationsurgery. Murdoch G, Jacobs NA, Wilson AB jr. Strathclyde:ISPO Int., University of Strathclyde.22. Functional capabilities of lower extremity amputees. KegelB, Carpenter ML, Burgess EM. Arch Phys Med Rehab, 59:109-120. 197823. Amputation surgery and rehabilitation, The Toronto experience.JP Kostuik, R Gillespie. Churchill Livingstone 1981.Ch 6 Below knee amputation 67-7324. Energy costs of walking amputees: the influence of level ofamputation. RL Waters. J Perry, D Antonelli, H Hislop J BoneJoint Surg Am, 1976;58:42-4625. A systematic review of outcomes and complications of reconstructionand amputation for type IIIB and IIIC fracturesof the tibia. D Saddawi-Konefka, BS Hyungjin Myra Kim, KCChung. Plastic and reconstructive surgery decmeber 2008.26. Complex limb salvage or early amputation for severe lower-limbinjury: A meta-analysis of observational studies.JW Busse, CL Jacobs, MF Swiontkowski, MJ Bosse, MHBhandarie. J Orthop Trauma 2007.27. A meta-analysis of amputation versus limb salvage inmangled lower limb injuries- The patient perspective.Injury 2010. Maheswara Akula, Sreenadh Gella, CJ Shaw, PMcShane, AM Mohsen28. Stump management after trans-tibial amputation: A systematicreview. Prosthetics and orthotics international 2005.SE Nawijn, H van der Linde, CH Emmelot, CJ Hofstad29. Complications following limb-threatening lower extremitytrauma. AH Harris, PL Althausen, J Kellam, MJ Bosse, RCastillo, LEAP study group. J Orthop trauma, januari 2009.30. Short-term wound complications after application of flapsfor coverage of traumatic sof-tissue defects about the tibia.AN Pollak, ML McCarthy, AR Burgess. J Bone Joint Surg Am.2000.31. Ability of lower-extremity injury severity scores to predictfunctional outcome after limb salvage. TV Ly, TG Travison,RC Castillo, MJ Bosse, EJ MacKenzie, LEAP study group. JBone Joint Surg Am. 2008.32. The utility of scores in the decisione to salvage or amputationof severely injued limbs. R Shanmuganathan. Indian JOrthop 200833. The mangeld foot and leg: salvage versus amputation. SBShawen, JJ Keeling, J Branstetter, KL Kirk, JR Ficke. FootAnkle Clin N Am 15(2010) 63-7534. Amputation und prothesenversorgung der unteren extremität.Baumgartner R, Bota P. Enke Verlag Stuttgart 1995.35. Amputation Versus Reconstruction in Traumatic Defects ofthe Leg: Outcome and Costs. Hertel, R. Strebel, N. Ganz, R.J Orthop Trauma 1996;10:223-22936. Grade III open tibial fractures: functional outcome andquality of life in amputees versus patients with successfulreconstruction. Hoogendoorn JM, van der Werken Chr.Injury 2001;32(May(4)):329-34178 ■ <strong>Nederlands</strong> <strong>Tijdschrift</strong> <strong>voor</strong> <strong>Orthopaedie</strong>, Vol 18, Nr 4, december 2011
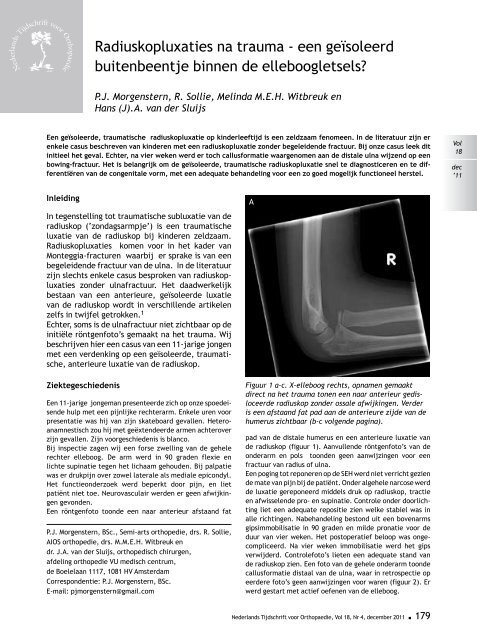
<strong>Nederlands</strong> <strong>Tijdschrift</strong><strong>voor</strong> <strong>Orthopaedie</strong>Radiuskopluxaties na trauma - een geïsoleerdbuitenbeentje binnen de elleboogletsels?P.J. Morgenstern, R. Sollie, Melinda M.E.H. Witbreuk enHans (J).A. van der SluijsEen geïsoleerde, traumatische radiuskopluxatie op kinderleeftijd is een zeldzaam fenomeen. In de literatuur zijn erenkele casus beschreven van kinderen met een radiuskopluxatie zonder begeleidende fractuur. Bij onze casus leek ditinitieel het geval. Echter, na vier weken werd er toch callusformatie waargenomen aan de distale ulna wijzend op eenbowing-fractuur. Het is belangrijk om de geïsoleerde, traumatische radiuskopluxatie snel te diagnosticeren en te differentiërenvan de congenitale vorm, met een adequate behandeling <strong>voor</strong> een zo goed mogelijk functioneel herstel.Vol18dec’11InleidingIn tegenstelling tot traumatische subluxatie van deradiuskop (‘zondagsarmpje’) is een traumatischeluxatie van de radiuskop bij kinderen zeldzaam.Radiuskopluxaties komen <strong>voor</strong> in het kader vanMonteggia-fracturen waarbij er sprake is van eenbegeleidende fractuur van de ulna. In de literatuurzijn slechts enkele casus besproken van radiuskopluxatieszonder ulnafractuur. Het daadwerkelijkbestaan van een anterieure, geïsoleerde luxatievan de radiuskop wordt in verschillende artikelenzelfs in twijfel getrokken. 1Echter, soms is de ulnafractuur niet zichtbaar op deinitiële röntgenfoto’s gemaakt na het trauma. Wijbeschrijven hier een casus van een 11-jarige jongenmet een verdenking op een geïsoleerde, traumatische,anterieure luxatie van de radiuskop.ZiektegeschiedenisEen 11-jarige jongeman presenteerde zich op onze spoedeisendehulp met een pijnlijke rechterarm. Enkele uren <strong>voor</strong>presentatie was hij van zijn skateboard gevallen. Heteroanamnestischzou hij met geëxtendeerde armen achteroverzijn gevallen. Zijn <strong>voor</strong>geschiedenis is blanco.Bij inspectie zagen wij een forse zwelling van de gehelerechter elleboog. De arm werd in 90 graden flexie enlichte supinatie tegen het lichaam gehouden. Bij palpatiewas er drukpijn over zowel laterale als mediale epicondyl.Het functieonderzoek werd beperkt door pijn, en lietpatiënt niet toe. Neurovasculair werden er geen afwijkingengevonden.Een röntgenfoto toonde een naar anterieur afstaand fatP.J. Morgenstern, BSc., Semi-arts orthopedie, drs. R. Sollie,AIOS orthopedie, drs. M.M.E.H. Witbreuk endr. J.A. van der Sluijs, orthopedisch chirurgen,afdeling orthopedie VU medisch centrum,de Boelelaan 1117, 1081 HV AmsterdamCorrespondentie: P.J. Morgenstern, BSc.E-mail: pjmorgenstern@gmail.comAFiguur 1 a-c. X-elleboog rechts, opnamen gemaaktdirect na het trauma tonen een naar anterieur gedisloceerderadiuskop zonder ossale afwijkingen. Verderis een afstaand fat pad aan de anterieure zijde van dehumerus zichtbaar (b-c volgende pagina).pad van de distale humerus en een anterieure luxatie vande radiuskop (figuur 1). Aanvullende röntgenfoto’s van deonderarm en pols toonden geen aanwijzingen <strong>voor</strong> eenfractuur van radius of ulna.Een poging tot reponeren op de SEH werd niet verricht geziende mate van pijn bij de patiënt. Onder algehele narcose werdde luxatie gereponeerd middels druk op radiuskop, tractieen afwisselende pro- en supinatie. Controle onder doorlichtingliet een adequate repositie zien welke stabiel was inalle richtingen. Nabehandeling bestond uit een bovenarmsgipsimmobilisatie in 90 graden en milde pronatie <strong>voor</strong> deduur van vier weken. Het postoperatief beloop was ongecompliceerd.Na vier weken immobilisatie werd het gipsverwijderd. Controlefoto’s lieten een adequate stand vande radiuskop zien. Een foto van de gehele onderarm toondecallusformatie distaal van de ulna, waar in retrospectie opeerdere foto’s geen aanwijzingen <strong>voor</strong> waren (figuur 2). Erwerd gestart met actief oefenen van de elleboog.<strong>Nederlands</strong> <strong>Tijdschrift</strong> <strong>voor</strong> <strong>Orthopaedie</strong>, Vol 18, Nr 4, december 2011 ■ 179



![NTvO OKT 2007 [ed_3].indd - Nederlands Tijdschrift voor Orthopaedie](https://img.yumpu.com/33045418/1/190x255/ntvo-okt-2007-ed-3indd-nederlands-tijdschrift-voor-orthopaedie.jpg?quality=85)