

kwartalnik polskiego towarzystwa ultrasonograficznego
kwartalnik polskiego towarzystwa ultrasonograficznego
kwartalnik polskiego towarzystwa ultrasonograficznego

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
arterial and portal venous / sinusoidal phase by contrast<br />
enhanced ultrasound allows for reliable differentiation<br />
between fnH and Hca. this important finding<br />
could be explained by the lack of portal veins in Hca in<br />
contrast to fnH which presents (atypical) portal veins<br />
in many but not all patients. fnH typically appears<br />
Characterization of focal liver lesions in non-cirrhotic liver<br />
as a hyper-perfused tumour-like lesion relative to the<br />
surrounding liver tissue in the arterial phase. During<br />
the portal venous phase fnH is slightly hyperechogenic<br />
in comparison to the surrounding liver parenchyma<br />
[figure 3].<br />
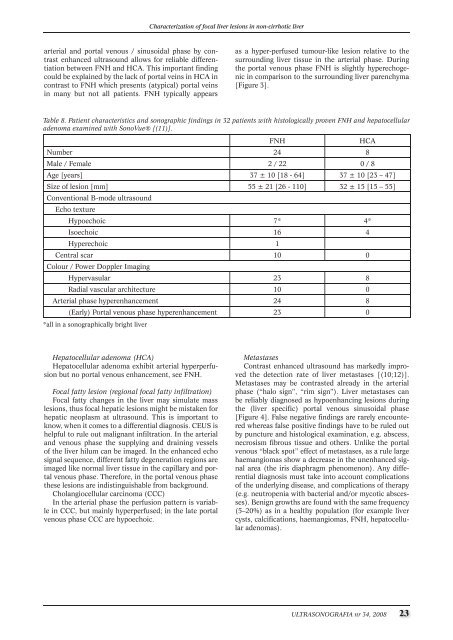
Table 8. Patient characteristics and sonographic findings in 32 patients with histologically proven FNH and hepatocellular<br />
adenoma examined with SonoVue® [(11)].<br />
fnH Hca<br />
number 24 8<br />
Male / female 2 / 22 0 / 8<br />
age [years] 37 ± 10 [18 - 64] 37 ± 10 [23 – 47]<br />
size of lesion [mm] 55 ± 21 [26 - 110] 32 ± 15 [15 – 55]<br />
conventional B-mode ultrasound<br />
Echo texture<br />
Hypoechoic 7* 4*<br />
Isoechoic 16 4<br />
Hyperechoic 1<br />
Central scar 10 0<br />
colour / Power Doppler imaging<br />
Hypervasular 23 8<br />
Radial vascular architecture 10 0<br />
Arterial phase hyperenhancement 24 8<br />
(Early) Portal venous phase hyperenhancement 23 0<br />
*all in a sonographically bright liver<br />
Hepatocellular adenoma (HCA)<br />
Hepatocellular adenoma exhibit arterial hyperperfusion<br />
but no portal venous enhancement, see fnH.<br />
Focal fatty lesion (regional focal fatty infiltration)<br />
focal fatty changes in the liver may simulate mass<br />
lesions, thus focal hepatic lesions might be mistaken for<br />
hepatic neoplasm at ultrasound. this is important to<br />
know, when it comes to a differential diagnosis. cEUs is<br />
helpful to rule out malignant infiltration. in the arterial<br />
and venous phase the supplying and draining vessels<br />
of the liver hilum can be imaged. in the enhanced echo<br />
signal sequence, different fatty degeneration regions are<br />
imaged like normal liver tissue in the capillary and portal<br />
venous phase. therefore, in the portal venous phase<br />
these lesions are indistinguishable from background.<br />
cholangiocellular carcinoma (ccc)<br />
in the arterial phase the perfusion pattern is variable<br />
in ccc, but mainly hyperperfused; in the late portal<br />
venous phase ccc are hypoechoic.<br />
Metastases<br />
contrast enhanced ultrasound has markedly improved<br />
the detection rate of liver metastases [(10;12)].<br />
Metastases may be contrasted already in the arterial<br />
phase (“halo sign”, “rim sign”). liver metastases can<br />
be reliably diagnosed as hypoenhancing lesions during<br />
the (liver specific) portal venous sinusoidal phase<br />
[figure 4]. false negative findings are rarely encountered<br />
whereas false positive findings have to be ruled out<br />
by puncture and histological examination, e.g. abscess,<br />
necrosism fibrous tissue and others. Unlike the portal<br />
venous “black spot” effect of metastases, as a rule large<br />
haemangiomas show a decrease in the unenhanced signal<br />
area (the iris diaphragm phenomenon). any differential<br />
diagnosis must take into account complications<br />
of the underlying disease, and complications of therapy<br />
(e.g. neutropenia with bacterial and/or mycotic abscesses).<br />
Benign growths are found with the same frequency<br />
(5–20%) as in a healthy population (for example liver<br />
cysts, calcifications, haemangiomas, fnH, hepatocellular<br />
adenomas).<br />
ULTRASONOGRAFIA nr 34, 2008 23
![Ultrasonografia nr21 [4.58 Mb] - Kwartalnik](https://img.yumpu.com/51838921/1/184x260/ultrasonografia-nr21-458-mb-kwartalnik.jpg?quality=85)
![Ultrasonografia nr35 [13.00 MB] - Kwartalnik](https://img.yumpu.com/10640460/1/188x260/ultrasonografia-nr35-1300-mb-kwartalnik.jpg?quality=85)
![Ultrasonografia nr39 [8.00 MB] - Kwartalnik](https://img.yumpu.com/10637726/1/188x260/ultrasonografia-nr39-800-mb-kwartalnik.jpg?quality=85)

![Ultrasonografia nr46 [3.17 Mb] - Kwartalnik](https://img.yumpu.com/6154909/1/188x260/ultrasonografia-nr46-317-mb-kwartalnik.jpg?quality=85)