

90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin

Erfolgreiche ePaper selbst erstellen
Machen Sie aus Ihren PDF Publikationen ein blätterbares Flipbook mit unserer einzigartigen Google optimierten e-Paper Software.
Intertrochantäre Varisationsosteotomie mit einem Korrekturwinkel von 20°<br />
Proximal varus osteotomy with a correction angle of 20°<br />
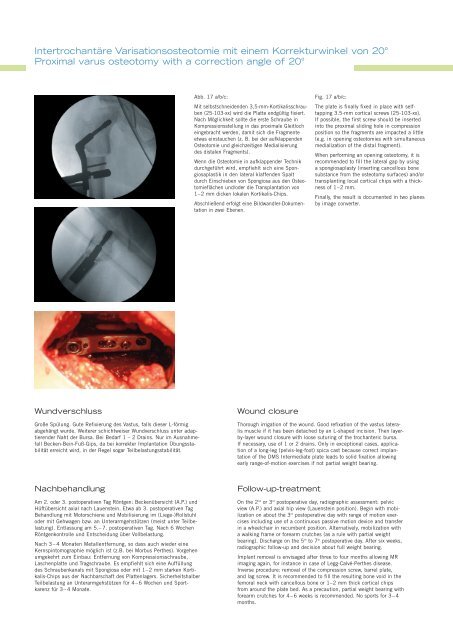
Abb. 17 a/b/c:<br />
Mit selbstschneidenden 3,5-mm-Kortikalisschrauben<br />
(25-103-xx) wird die Platte endgültig fixiert.<br />
Nach Möglichkeit sollte die erste Schraube in<br />
Kompressionsstellung in das proximale Gleitloch<br />
eingebracht werden, damit sich die Fragmente<br />
etwas einstauchen (z. B. bei der aufklappenden<br />
Osteotomie und gleichzeitigen Medialisierung<br />
des distalen Fragments).<br />
Wenn die Osteotomie in aufklappender Technik<br />
durchgeführt wird, empfiehlt sich eine Spongiosaplastik<br />
in den lateral klaffenden Spalt<br />
durch Einschieben von Spongiosa aus den Osteotomieflächen<br />
und/oder die Transplantation von<br />
1–2 mm dicken lokalen Kortikalis-Chips.<br />
Abschließend erfolgt eine Bildwandler-Dokumentation<br />
in zwei Ebenen.<br />
Fig. 17 a/b/c:<br />
The plate is finally fixed in place with selftapping<br />
3.5-mm cortical screws (25-103-xx).<br />
If possible, the first screw should be inserted<br />
into the proximal sliding hole in compression<br />
position so the fragments are impacted a little<br />
(e.g. in opening osteotomies with simultaneous<br />
medialization of the distal fragment).<br />
When performing an opening osteotomy, it is<br />
recommended to fill the lateral gap by using<br />
a spongiosaplasty (inserting cancellous bone<br />
substance from the osteotomy surfaces) and/or<br />
transplanting local cortical chips with a thickness<br />
of 1–2 mm.<br />
Finally, the result is documented in two planes<br />
by image converter.<br />
Wundverschluss<br />
Große Spülung. Gute Refixierung des Vastus, falls dieser L-förmig<br />
abgehängt wurde. Weiterer schichtweiser Wundverschluss unter adaptierender<br />
Naht der Bursa. Bei Bedarf 1 – 2 Drains. Nur im Ausnahmefall<br />
Becken-Bein-Fuß-Gips, da bei korrekter Implantation Übungsstabilität<br />
erreicht wird, in der Regel sogar Teilbelastungsstabilität.<br />
Wound closure<br />
Thorough irrigation of the wound. Good refixation of the vastus lateralis<br />
muscle if it has been detached by an L-shaped incision. Then layerby-layer<br />
wound closure with loose suturing of the trochanteric bursa.<br />
If necessary, use of 1 or 2 drains. Only in exceptional cases, application<br />
of a long-leg (pelvis-leg-foot) spica cast because correct implantation<br />
of the DMS Intermediate plate leads to solid fixation allowing<br />
early range-of-motion exercises if not partial weight bearing.<br />
Nachbehandlung<br />
Am 2. oder 3. postoperativen Tag Röntgen: Beckenübersicht (A.P.) und<br />
Hüftübersicht axial nach Lauenstein. Etwa ab 3. postoperativen Tag<br />
Behandlung mit Motorschiene und Mobilisierung im (Liege-)Rollstuhl<br />
oder mit Gehwagen bzw. an Unterarmgehstützen (meist unter Teilbelastung).<br />
Entlassung am 5.–7. postoperativen Tag. Nach 6 Wochen<br />
Röntgenkontrolle und Entscheidung über Vollbelastung.<br />
Nach 3–4 Monaten Metallentfernung, so dass auch wieder eine<br />
Kernspintomographie möglich ist (z.B. bei Morbus Perthes). Vorgehen<br />
umgekehrt zum Einbau: Entfernung von Kompressionsschraube,<br />
Laschenplatte und Tragschraube. Es empfiehlt sich eine Auffüllung<br />
des Schraubenkanals mit Spongiosa oder mit 1–2 mm starken Kortikalis-Chips<br />
aus der Nachbarschaft des Plattenlagers. Sicherheitshalber<br />
Teilbelastung an Unterarmgehstützen für 4–6 Wochen und Sportkarenz<br />
für 3–4 Monate.<br />
Follow-up-treatment<br />
On the 2 nd or 3 rd postoperative day, radiographic assessment: pelvic<br />
view (A.P.) and axial hip view (Lauenstein position). Begin with mobilization<br />
on about the 3 rd postoperative day with range of motion exercises<br />
including use of a continuous passive motion device and transfer<br />
in a wheelchair in recumbent position. Alternatively, mobilization with<br />
a walking frame or forearm crutches (as a rule with partial weight<br />
bearing). Discharge on the 5 th to 7 th postoperative day. After six weeks,<br />
radiographic follow-up and decision about full weight bearing.<br />
Implant removal is envisaged after three to four months allowing MR<br />
imaging again, for instance in case of Legg-Calvé-Perthes disease.<br />
Inverse procedure: removal of the compression screw, barrel plate,<br />
and lag screw. It is recommended to fill the resulting bone void in the<br />
femoral neck with cancellous bone or 1–2 mm thick cortical chips<br />
from around the plate bed. As a precaution, partial weight bearing with<br />
forearm crutches for 4–6 weeks is recommended. No sports for 3–4<br />
months.













