

90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
3 Hole<br />
4 Hole<br />
6 Hole<br />
8 Hole<br />
25-178-04<br />
25-178-06<br />
25-178-08<br />
Gebrüder <strong>Martin</strong> GmbH & Co. KG<br />
A company of the <strong>KLS</strong> <strong>Martin</strong> Group · Ludwigstaler Str. 132 · D-78532 Tuttlingen · Postfach 60 · D-785<strong>01</strong> Tuttlingen<br />
Tel. +49 7461 706-0 · Fax +49 7461 706-193 · info@klsmartin.com · www.klsmartin.com<br />
3 Hole<br />
4 Hole<br />
6 Hole<br />
8 Hole<br />
Gebrüder <strong>Martin</strong> GmbH & Co. KG<br />
A company of the <strong>KLS</strong> <strong>Martin</strong> Group · Ludwigstaler Str. 132 · D-78532 Tuttlingen · Postfach 60 · D-785<strong>01</strong> Tuttlingen<br />
Tel. +49 7461 706-0 · Fax +49 7461 706-193 · info@klsmartin.com · www.klsmartin.com<br />
Intertrochantäre Varisationsosteotomie mit einem Korrekturwinkel von 20°<br />
Intertrochanteric varus osteotomy with a correction angle of 20°<br />
Präoperative Planung der<br />
Korrekturosteotomie<br />
Preoperative planning of<br />
the corrective osteotomy<br />
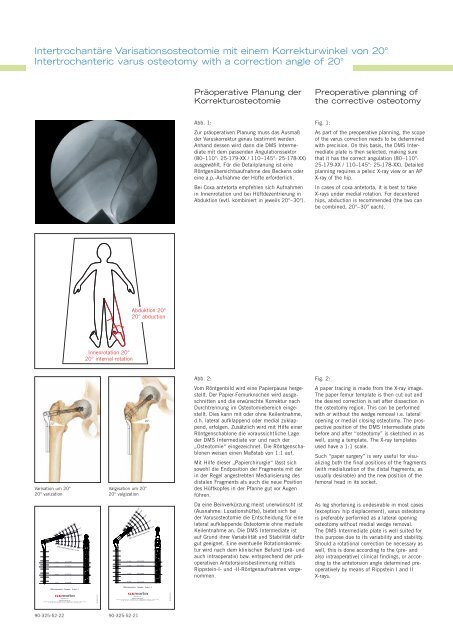
Abb. 1:<br />
Zur präoperativen Planung muss das Ausmaß<br />
der Varuskorrektur genau bestimmt werden.<br />
Anhand dessen wird dann die DMS Intermediate<br />
mit dem passenden Angulationssektor<br />
(80–110°: 25-179-XX / 110–145°: 25-178-XX)<br />
ausgewählt. Für die Detailplanung ist eine<br />
Röntgenübersichtsaufnahme des Beckens oder<br />
eine a.p.-Aufnahme der Hüfte erforderlich.<br />
Bei Coxa antetorta empfehlen sich Aufnahmen<br />
in Innenrotation und bei Hüftdezentrierung in<br />
Abduktion (evtl. kombiniert in jeweils 20°–30°).<br />
Fig. 1:<br />
As part of the preoperative planning, the scope<br />
of the varus correction needs to be determined<br />
with precision. On this basis, the DMS Intermediate<br />
plate is then selected, making sure<br />
that it has the correct angulation (80–110°:<br />
25-179-XX / 110–145°: 25-178-XX). Detailed<br />
planning requires a pelvic X-ray view or an AP<br />
X-ray of the hip.<br />
In cases of coxa antetorta, it is best to take<br />
X-rays under medial rotation. For decentered<br />
hips, abduction is recommended (the two can<br />
be combined, 20°–30° each).<br />
Abduktion 20°<br />
20° abduction<br />
Innenrotation 20°<br />
20° internal rotation<br />
Abb. 2:<br />
Vom Röntgenbild wird eine Papierpause hergestellt.<br />
Der Papier-Femurknochen wird ausgeschnitten<br />
und die erwünschte Korrektur nach<br />
Durchtrennung im Osteotomiebereich eingestellt.<br />
Dies kann mit oder ohne Keilentnahme,<br />
d.h. lateral aufklappend oder medial zuklappend,<br />
erfolgen. Zusätzlich wird mit Hilfe einer<br />
Röntgenschablone die voraussichtliche Lage<br />
der DMS Intermediate vor und nach der<br />
„Osteotomie“ eingezeichnet. Die Röntgenschablonen<br />
weisen einen Maßstab von 1:1 auf.<br />
Mit Hilfe dieser „Papierchirurgie“ lässt sich<br />
sowohl die Endposition der Fragmente mit der<br />
in der Regel angestrebten Medialisierung des<br />
distalen Fragments als auch die neue Position<br />
des Hüftkopfes in der Pfanne gut vor Augen<br />
führen.<br />
Da eine Beinverkürzung meist unerwünscht ist<br />
(Ausnahme: Luxationshüfte), bietet sich bei<br />
der Varusosteotomie die Entscheidung für eine<br />
lateral aufklappende Osteotomie ohne mediale<br />
Keilentnahme an. Die DMS Intermediate ist<br />
auf Grund ihrer Variabilität und Stabilität dafür<br />
gut geeignet. Eine eventuelle Rotationskorrektur<br />
wird nach dem klinischen Befund (prä- und<br />
auch intraoperativ) bzw. entsprechend der präoperativen<br />
Antetorsionsbestimmung mittels<br />
Rippstein-I- und -II-Röntgenaufnahmen vorgenommen.<br />
Fig. 2:<br />
A paper tracing is made from the X-ray image.<br />
The paper femur template is then cut out and<br />
the desired correction is set after dissection in<br />
the osteotomy region. This can be performed<br />
with or without the wedge removal i.e. lateral<br />
opening or medial closing osteotomy. The prospective<br />
position of the DMS Intermediate plate<br />
before and after “osteotomy” is sketched in as<br />
well, using a template. The X-ray templates<br />
used have a 1:1 scale.<br />
Such “paper surgery” is very useful for visualizing<br />
both the final positions of the fragments<br />
(with medialization of the distal fragments, as<br />
usually desirable) and the new position of the<br />
femoral head in its socket.<br />
20°<br />
Varisation um 20°<br />
20° varization<br />
Valgisation um 20°<br />
20° valgization<br />
20°<br />
35 40 50 60 70 80 <strong>90</strong> 100<br />
110°<br />
100°<br />
<strong>90</strong>°<br />
35 40 50 60 70 80 <strong>90</strong> 100 80°<br />
DMS intermediate lag screw<br />
25-178-03<br />
3540 50 60 70 80 <strong>90</strong> 100<br />
145°<br />
140°<br />
130°<br />
120°<br />
35 40 50 60 70 80 <strong>90</strong> 100<br />
DMS intermediate lag screw<br />
25-179-03<br />
25-179-04<br />
25-179-06<br />
110°<br />
As leg shortening is undesirable in most cases<br />
(exception: hip displacement), varus osteotomy<br />
is preferably performed as a lateral opening<br />
osteotomy without medial wedge removal.<br />
The DMS Intermediate plate is well suited for<br />
this purpose due to its variability and stability.<br />
Should a rotational correction be necessary as<br />
well, this is done according to the (pre- and<br />
also intraoperative) clinical findings, or according<br />
to the antetorsion angle determined preoperatively<br />
by means of Rippstein I and II<br />
X-rays.<br />
25-179-08<br />
DMS intermediate - Template Scale 1:1<br />
DMS intermediate - Template Scale 1:1<br />
<strong>90</strong>-325-52-21<br />
<strong>90</strong>-325-52-22<br />
<strong>90</strong>-325-52-22 <strong>90</strong>-325-52-21













