

90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
Fall 2<br />
Case 2<br />
Epiphyseolysis capitis femoris links,<br />
Grad III<br />
Späte Erstverstellung. Zunächst subkapitale Osteotomie<br />
nach Dunn-Fish mit begrenzter Aufrichtung des Kopfes.<br />
Verzögerte knöcherne Konsolidierung bei eingeschränkter<br />
Compliance (viel zu frühe Vollbelastung).<br />
Keine Entwicklung einer Kopfnekrose. Beinlängendifferenz<br />
(- 2,5 cm links). Femoroazetabuläres Impingement.<br />
16-jähriger Junge. 66 kg Körpergewicht.<br />
Slipped upper femoral epiphysis<br />
on the left, grade III<br />
Late presentation. Initial treatment by subcapital cuneiform<br />
osteotomy according to Dunn-Fish with limited correction.<br />
Delayed bony consolidation because of poor compliance<br />
(early full weight bearing). Fortunately no development of<br />
a vascular necrosis. Leg length discrepancy (- 2.5 cm on<br />
the left). Femoroacetabular impingement.<br />
16-year-old boy. 66 kg body weight at operation.<br />
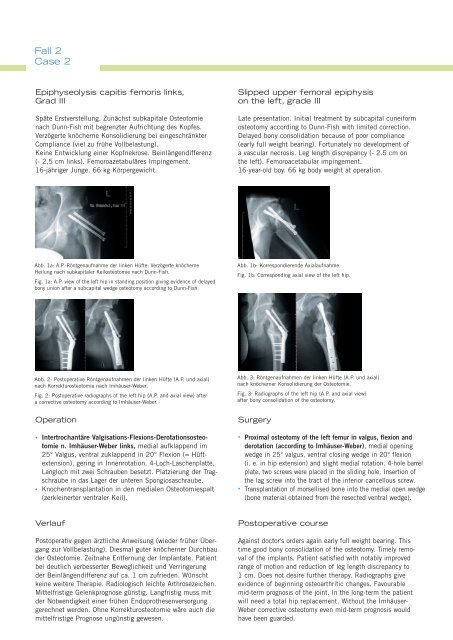
Abb. 1a: A.P.-Röntgenaufnahme der linken Hüfte: Verzögerte knöcherne<br />
Heilung nach subkapitaler Keilosteotomie nach Dunn-Fish.<br />
Fig. 1a: A.P. view of the left hip in standing position giving evidence of delayed<br />
bony union after a subcapital wedge osteotomy according to Dunn-Fish.<br />
Abb. 1b: Korrespondierende Axialaufnahme.<br />
Fig. 1b: Corresponding axial view of the left hip.<br />
Abb. 2: Postoperative Röntgenaufnahmen der linken Hüfte (A.P. und axial)<br />
nach Korrekturosteotomie nach Imhäuser-Weber.<br />
Fig. 2: Postoperative radiographs of the left hip (A.P. and axial view) after<br />
a corrective osteotomy according to Imhäuser-Weber.<br />
Operation<br />
• Intertrochantäre Valgisations-Flexions-Derotationsosteotomie<br />
n. Imhäuser-Weber links, medial aufklappend im<br />
25° Valgus, ventral zuklappend in 20° Flexion (= Hüftextension),<br />
gering in Innenrotation. 4-Loch-Laschenplatte,<br />
Langloch mit zwei Schrauben besetzt. Platzierung der Tragschraube<br />
in das Lager der unteren Spongiosaschraube.<br />
• Knochentransplantation in den medialen Osteotomiespalt<br />
(zerkleinerter ventraler Keil).<br />
Abb. 3: Röntgenaufnahmen der linken Hüfte (A.P. und axial)<br />
nach knöcherner Konsolidierung der Osteotomie.<br />
Fig. 3: Radiographs of the left hip (A.P. and axial view)<br />
after bony consolidation of the osteotomy.<br />
Surgery<br />
• Proximal osteotomy of the left femur in valgus, flexion and<br />
derotation (according to Imhäuser-Weber), medial opening<br />
wedge in 25° valgus, ventral closing wedge in 20° flexion<br />
(i. e. in hip extension) and slight medial rotation. 4-hole barrel<br />
plate, two screws were placed in the sliding hole. Insertion of<br />
the lag screw into the tract of the inferior cancellous screw.<br />
• Transplantation of morsellised bone into the medial open wedge<br />
(bone material obtained from the resected ventral wedge).<br />
Verlauf<br />
Postoperativ gegen ärztliche Anweisung (wieder früher Übergang<br />
zur Vollbelastung). Diesmal guter knöcherner Durchbau<br />
der Osteotomie. Zeitnahe Entfernung der Implantate. Patient<br />
bei deutlich verbesserter Beweglichkeit und Verringerung<br />
der Beinlängendifferenz auf ca. 1 cm zufrieden. Wünscht<br />
keine weitere Therapie. Radiologisch leichte Arthrosezeichen.<br />
Mittelfristige Gelenkprognose günstig. Langfristig muss mit<br />
der Notwendigkeit einer frühen Endoprothesenversorgung<br />
gerechnet werden. Ohne Korrekturosteotomie wäre auch die<br />
mittelfristige Prognose ungünstig gewesen.<br />
Postoperative course<br />
Against doctor's orders again early full weight bearing. This<br />
time good bony consolidation of the osteotomy. Timely removal<br />
of the implants. Patient satisfied with notably improved<br />
range of motion and reduction of leg length discrepancy to<br />
1 cm. Does not desire further therapy. Radiographs give<br />
evidence of beginning osteoarthritic changes. Favourable<br />
mid-term prognosis of the joint. In the long-term the patient<br />
will need a total hip replacement. Without the Imhäuser-<br />
Weber corrective osteotomy even mid-term prognosis would<br />
have been guarded.













