

90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin
90-269-01 MicroStop dt.qxd - KLS Martin

Sie wollen auch ein ePaper? Erhöhen Sie die Reichweite Ihrer Titel.
YUMPU macht aus Druck-PDFs automatisch weboptimierte ePaper, die Google liebt.
Intertrochantäre Varisationsosteotomie mit einem Korrekturwinkel von 20°<br />
Intertrochanteric varus osteotomy with a correction angle of 20°<br />
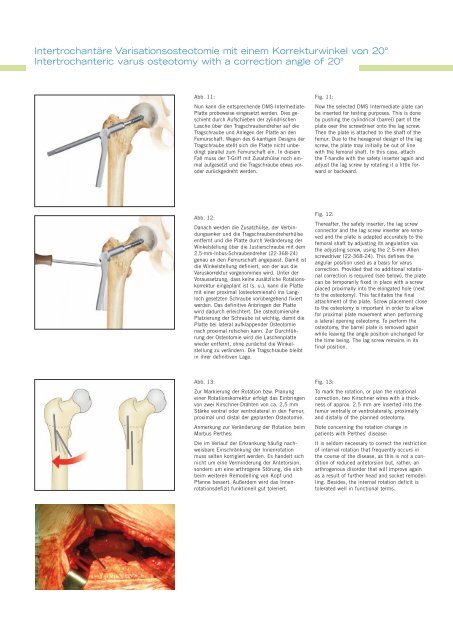
Abb. 11:<br />
Nun kann die entsprechende DMS-Intermediate-<br />
Platte probeweise eingesetzt werden. Dies geschieht<br />
durch Aufschieben der zylindrischen<br />
Lasche über den Tragschraubendreher auf die<br />
Tragschraube und Anlegen der Platte an den<br />
Femurschaft. Wegen des 6-kantigen Designs der<br />
Tragschraube stellt sich die Platte nicht unbedingt<br />
parallel zum Femurschaft ein. In diesem<br />
Fall muss der T-Griff mit Zusatzhülse noch einmal<br />
aufgesetzt und die Tragschraube etwas voroder<br />
zurückgedreht werden.<br />
Fig. 11:<br />
Now the selected DMS Intermediate plate can<br />
be inserted for testing purposes. This is done<br />
by pushing the cylindrical (barrel) part of the<br />
plate over the screwdriver onto the lag screw.<br />
Then the plate is attached to the shaft of the<br />
femur. Due to the hexagonal design of the lag<br />
screw, the plate may initially be out of line<br />
with the femoral shaft. In this case, attach<br />
the T-handle with the safety inserter again and<br />
adjust the lag screw by rotating it a little forward<br />
or backward.<br />
Abb. 12:<br />
Danach werden die Zusatzhülse, der Verbindungsanker<br />
und die Tragschraubendreherhülse<br />
entfernt und die Platte durch Veränderung der<br />
Winkelstellung über die Justierschraube mit dem<br />
2,5-mm-Inbus-Schraubendreher (22-368-24)<br />
genau an den Femurschaft angepasst. Damit ist<br />
die Winkelstellung definiert, von der aus die<br />
Varuskorrektur vorgenommen wird. Unter der<br />
Voraussetzung, dass keine zusätzliche Rotationskorrektur<br />
eingeplant ist (s. u.), kann die Platte<br />
mit einer proximal (osteotomienah) ins Langloch<br />
gesetzten Schraube vorübergehend fixiert<br />
werden. Das definitive Anbringen der Platte<br />
wird dadurch erleichtert. Die osteotomienahe<br />
Platzierung der Schraube ist wichtig, damit die<br />
Platte bei lateral aufklappender Osteotomie<br />
nach proximal rutschen kann. Zur Durchführung<br />
der Osteotomie wird die Laschenplatte<br />
wieder entfernt, ohne zunächst die Winkelstellung<br />
zu verändern. Die Tragschraube bleibt<br />
in ihrer definitiven Lage.<br />
Fig. 12:<br />
Thereafter, the safety inserter, the lag screw<br />
connector and the lag screw inserter are removed<br />
and the plate is adapted accurately to the<br />
femoral shaft by adjusting its angulation via<br />
the adjusting screw, using the 2.5-mm Allen<br />
screwdriver (22-368-24). This defines the<br />
angular position used as a basis for varus<br />
correction. Provided that no additional rotational<br />
correction is required (see below), the plate<br />
can be temporarily fixed in place with a screw<br />
placed proximally into the elongated hole (next<br />
to the osteotomy). This facilitates the final<br />
attachment of the plate. Screw placement close<br />
to the osteotomy is important in order to allow<br />
for proximal plate movement when performing<br />
a lateral opening osteotomy. To perform the<br />
osteotomy, the barrel plate is removed again<br />
while leaving the angle position unchanged for<br />
the time being. The lag screw remains in its<br />
final position.<br />
Abb. 13:<br />
Zur Markierung der Rotation bzw. Planung<br />
einer Rotationskorrektur erfolgt das Einbringen<br />
von zwei Kirschner-Drähten von ca. 2,5 mm<br />
Stärke ventral oder ventrolateral in den Femur,<br />
proximal und distal der geplanten Osteotomie.<br />
Anmerkung zur Veränderung der Rotation beim<br />
Morbus Perthes:<br />
Die im Verlauf der Erkrankung häufig nachweisbare<br />
Einschränkung der Innenrotation<br />
muss selten korrigiert werden. Es handelt sich<br />
nicht um eine Verminderung der Antetorsion,<br />
sondern um eine arthrogene Störung, die sich<br />
beim weiteren Remodelling von Kopf und<br />
Pfanne bessert. Außerdem wird das Innenrotationsdefizit<br />
funktionell gut toleriert.<br />
Fig. 13:<br />
To mark the rotation, or plan the rotational<br />
correction, two Kirschner wires with a thickness<br />
of approx. 2.5 mm are inserted into the<br />
femur ventrally or ventrolaterally, proximally<br />
and distally of the planned osteotomy.<br />
Note concerning the rotation change in<br />
patients with Perthes’ disease:<br />
It is seldom necessary to correct the restriction<br />
of internal rotation that frequently occurs in<br />
the course of the disease, as this is not a condition<br />
of reduced antetorsion but, rather, an<br />
arthrogenous disorder that will improve again<br />
as a result of further head and socket remodelling.<br />
Besides, the internal rotation deficit is<br />
tolerated well in functional terms.













