

DM Full Guideline (2010) - VA/DoD Clinical Practice Guidelines Home
DM Full Guideline (2010) - VA/DoD Clinical Practice Guidelines Home
DM Full Guideline (2010) - VA/DoD Clinical Practice Guidelines Home

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Version 4.0<br />
<strong>VA</strong>/<strong>DoD</strong> <strong>Clinical</strong> <strong>Practice</strong> <strong>Guideline</strong><br />
for the Management of Diabetes Mellitus<br />
LIPID PHARMACOTHERAPY:<br />
18. Statins are first line agents in primary and secondary prevention of CVD regardless of HDL-C or TG level. [A]<br />
19. Moderate doses of formulary statins (to achieve an LDL-C reduction of 25% or greater) should be initiated<br />
unless a patient is considered to be at greater than usual risk for adverse events from statins (e.g., myopathy).<br />
[A]<br />
20. For patients who cannot tolerate statins, niacin or resins should be considered for treatment. [ A ]<br />
21. There is insufficient clinical outcome evidence to recommend ezetimibe monotherapy for reduction of CV risk.<br />
[ I ]<br />
22. Ezetimibe can be considered for lowering LDL-C in patients who are unable to tolerate other lipid-lowering<br />
drugs, or in combination with other drugs. [A]<br />
23. The dose of statin should be adjusted at 6 to 12 week intervals until individual LDL-C goals are achieved or<br />
statin doses have been maximized. [ I ]<br />
Isolated Hypertriglyceridemia<br />
24. Niacin, fibrates, or fish oil (omega-3 fatty acids) supplements may be used in treatment of isolated<br />
hypertriglyceridemia. [ B ]<br />
Isolated Low HDL-C<br />
25. For secondary prevention gemfibrozil or niacin may be used in patients with isolated low HDL-C and normal<br />
LDL-C. [A-Gemfibrozil; B-Niacin]<br />
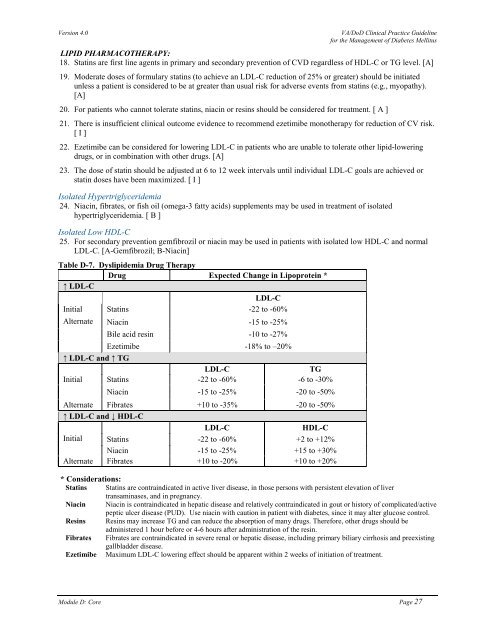
Table D-7. Dyslipidemia Drug Therapy<br />
Drug Expected Change in Lipoprotein *<br />
↑ LDL-C<br />
LDL-C<br />
Initial Statins -22 to -60%<br />
Alternate Niacin -15 to -25%<br />
Bile acid resin -10 to -27%<br />
Ezetimibe -18% to –20%<br />
↑ LDL-C and ↑ TG<br />
LDL-C<br />
TG<br />
Initial Statins -22 to -60% -6 to -30%<br />
Niacin -15 to -25% -20 to -50%<br />
Alternate Fibrates +10 to -35% -20 to -50%<br />
↑ LDL-C and ↓ HDL-C<br />
LDL-C<br />
HDL-C<br />
Initial Statins -22 to -60% +2 to +12%<br />
Niacin -15 to -25% +15 to +30%<br />
Alternate Fibrates +10 to -20% +10 to +20%<br />
* Considerations:<br />
Statins Statins are contraindicated in active liver disease, in those persons with persistent elevation of liver<br />
transaminases, and in pregnancy.<br />
Niacin Niacin is contraindicated in hepatic disease and relatively contraindicated in gout or history of complicated/active<br />
peptic ulcer disease (PUD). Use niacin with caution in patient with diabetes, since it may alter glucose control.<br />
Resins Resins may increase TG and can reduce the absorption of many drugs. Therefore, other drugs should be<br />
administered 1 hour before or 4-6 hours after administration of the resin.<br />
Fibrates Fibrates are contraindicated in severe renal or hepatic disease, including primary biliary cirrhosis and preexisting<br />
gallbladder disease.<br />
Ezetimibe Maximum LDL-C lowering effect should be apparent within 2 weeks of initiation of treatment.<br />
Module D: Core Page 27













