

Full document - International Hospital Federation
Full document - International Hospital Federation
Full document - International Hospital Federation

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Innovation and clinical specialities: burns<br />
challenging to splint, with various<br />
materials used for “airplane<br />
splints”. Because splinting in<br />
abduction can be uncomfortable<br />
and awkward, this is sometimes<br />
neglected. However, the inability to<br />
abduct the arms leads to<br />
Figure 6: Position of safety<br />
significant morbidity, and it severely<br />
for splinting hands 59<br />
limits overhead activities. 53<br />
The ankle can have contractures in both directions. Burns and<br />
scar contractures to the dorsum are more common, which must<br />
be combated with plantar flexion exercises and splints. However,<br />
the Achilles tendon may also become shortened with a prolonged<br />
planter flexion. For an ambulating patient, this is not a concern.<br />
However, for a patient who is bed-ridden, splinting should be<br />
initially for dorsiflexion to prevent Achilles tendon shortening.<br />
Fingers and hands should be splinted in the position of safety<br />
(Figure 6), with MCPs flexed and IPs extended. If there is a severe<br />
burn over the palmer aspect of the MCP joints, the MP joints can<br />
sometimes be splinted in extension, but it becomes very important<br />
to ensure that daily exercises maintain good flexion of the collateral<br />
ligaments of the MCP joint, which can tighten when in extension.<br />
Oral burns, particularly commissure burns can lead to<br />
complications of microstomia. These can be initially managed with<br />
mouth exercises, and gradually increasing the amount of mouth<br />
opening.Splints can also be fabricated to stretch the<br />
commissures. 54<br />
Surgical release<br />
Surgical release of burn contractures can involve local flaps for<br />
reorientation of the scar, but often also include a skin deficit which<br />
must be filled with a graft or flap. Skin grafts are also more prone<br />
to contractures, and aggressive post-operative therapy much be<br />
implemented. Repeat surgeries may be necessary. Thick (full<br />
thickness if the area is small enough) unmeshed grafts offer less<br />
contracture. Alternatives include artificial dermal substitutes that<br />
will allow decreased contracture with thinner split-thickness grafts.<br />
However, dermal substitutes such as Integra, a bovine collagen<br />
product, are commercial produced and extremely expensive. If<br />
skin or myocutaneous flaps are possible, they offer the advantage<br />
of coverage with minimal contracture and need for repeat surgery.<br />
These include both local flaps such as z-plasties and transposition<br />
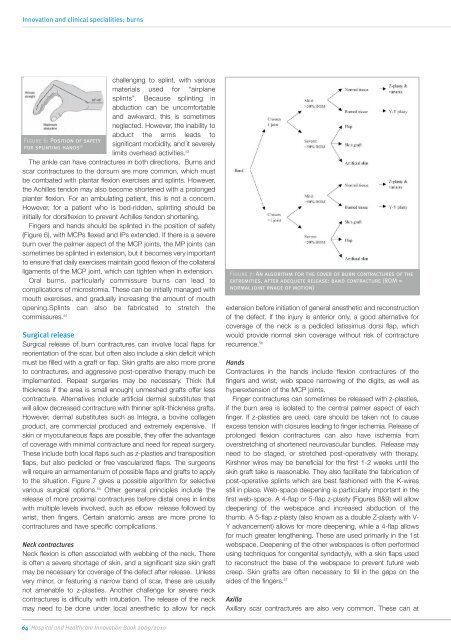
flaps, but also pedicled or free vascularized flaps. The surgeons<br />
will require an armamentarium of possible flaps and grafts to apply<br />
to the situation. Figure 7 gives a possible algorithm for selective<br />
various surgical options. 55 Other general principles include the<br />
release of more proximal contractures before distal ones in limbs<br />
with multiple levels involved, such as elbow release followed by<br />
wrist, then fingers. Certain anatomic areas are more prone to<br />
contractures and have specific complications.<br />
Neck contractures<br />
Neck flexion is often associated with webbing of the neck. There<br />
is often a severe shortage of skin, and a significant size skin graft<br />
may be necessary for coverage of the defect after release. Unless<br />
very minor, or featuring a narrow band of scar, these are usually<br />
not amenable to z-plasties. Another challenge for severe neck<br />
contractures is difficulty with intubation. The release of the neck<br />
may need to be done under local anesthetic to allow for neck<br />
Figure 7: An algorithm for the cover of burn contractures of the<br />
extremities, after adequete release: band contracture (ROM =<br />
normal joint rnage of motion)<br />
extension before initiation of general anesthetic and reconstruction<br />
of the defect. If the injury is anterior only, a good alternative for<br />
coverage of the neck is a pedicled latissimus dorsi flap, which<br />
would provide normal skin coverage without risk of contracture<br />
recurrence. 56<br />
Hands<br />
Contractures in the hands include flexion contractures of the<br />
fingers and wrist, web space narrowing of the digits, as well as<br />
hyperextension of the MCP joints.<br />
Finger contractures can sometimes be released with z-plasties,<br />
if the burn area is isolated to the central palmer aspect of each<br />
finger. If z-plasties are used, care should be taken not to cause<br />
excess tension with closures leading to finger ischemia. Release of<br />
prolonged flexion contractures can also have ischemia from<br />
overstretching of shortened neurovascular bundles. Release may<br />
need to be staged, or stretched post-operatively with therapy.<br />
Kirshner wires may be beneficial for the first 1-2 weeks until the<br />
skin graft take is reasonable. They also facilitate the fabrication of<br />
post-operative splints which are best fashioned with the K-wires<br />
still in place. Web-space deepening is particularly important in the<br />
first web-space. A 4-flap or 5-flap z-plasty (Figures 8&9) will allow<br />
deepening of the webspace and increased abduction of the<br />
thumb. A 5-flap z-plasty (also known as a double Z-plasty with V-<br />
Y advancement) allows for more deepening, while a 4-flap allows<br />
for much greater lengthening. These are used primarily in the 1st<br />
webspace. Deepening of the other webspaces is often performed<br />
using techniques for congenital syndactyly, with a skin flaps used<br />
to reconstruct the base of the webspace to prevent future web<br />
creep. Skin grafts are often necessary to fill in the gaps on the<br />
sides of the fingers. 57<br />
Axilla<br />
Axillary scar contractures are also very common. These can at<br />
64 <strong>Hospital</strong> and Healthcare Innovation Book 2009/2010














