

Clinical Guidelines for Acute Stroke Management - Living on the EDge
Clinical Guidelines for Acute Stroke Management - Living on the EDge
Clinical Guidelines for Acute Stroke Management - Living on the EDge

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
this test. Doppler ultrasound is widely available and<br />
useful in most centres. N<strong>on</strong> invasive measures <str<strong>on</strong>g>for</str<strong>on</strong>g><br />
symptomatic events were much less accurate <str<strong>on</strong>g>for</str<strong>on</strong>g><br />
patients with 50-70% stenosis, however, too few<br />
data exist and no clear c<strong>on</strong>clusi<strong>on</strong>s can be made. 102<br />
Carotid surgery is most beneficial early after n<strong>on</strong>severely<br />
disabling stroke (see secti<strong>on</strong> 7.7) and hence<br />
carotid imaging should be undertaken as part of <strong>the</strong><br />
initial diagnostic workup in selected patients.<br />
C. Cardiac imaging<br />
Echocardiography may be c<strong>on</strong>sidered to determine a<br />
potential cardioembolic source in selected patients<br />
(e.g. history of cardiac abnormalities or an abnormal<br />
electrocardiogram where <strong>the</strong>re are no current<br />
indicati<strong>on</strong>s <str<strong>on</strong>g>for</str<strong>on</strong>g> anticoagulati<strong>on</strong> or in patients with<br />
stroke of unknown origin after standard diagnostic<br />
workup). 116 Transthoracic echocardiography (TTE) is<br />
less invasive but less sensitive than transesophageal<br />
echocardiography (TEE) in detecting sources of<br />
cardiac emboli in patients with TIA or stroke. 116 TEE<br />
also appears more useful than TTE in assisting clinical<br />
decisi<strong>on</strong> making (i.e. aid decisi<strong>on</strong> whe<strong>the</strong>r to<br />
commence anticoagulati<strong>on</strong> or not). 117<br />
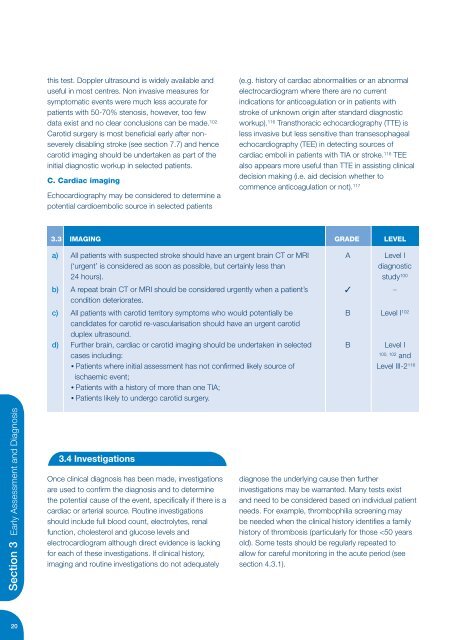
3.3 IMAGING GRADE LEVEL<br />
a) All patients with suspected stroke should have an urgent brain CT or MRI A Level I<br />
(‘urgent’ is c<strong>on</strong>sidered as so<strong>on</strong> as possible, but certainly less than<br />
diagnostic<br />
24 hours). study 100<br />
b) A repeat brain CT or MRI should be c<strong>on</strong>sidered urgently when a patient’s ✓ –<br />
c<strong>on</strong>diti<strong>on</strong> deteriorates.<br />
c) All patients with carotid territory symptoms who would potentially be B Level I 102<br />
candidates <str<strong>on</strong>g>for</str<strong>on</strong>g> carotid re-vascularisati<strong>on</strong> should have an urgent carotid<br />
duplex ultrasound.<br />
d) Fur<strong>the</strong>r brain, cardiac or carotid imaging should be undertaken in selected B Level I<br />
cases including:<br />
100, 102<br />
and<br />
• Patients where initial assessment has not c<strong>on</strong>firmed likely source of Level III-2 116<br />
ischaemic event;<br />
• Patients with a history of more than <strong>on</strong>e TIA;<br />
• Patients likely to undergo carotid surgery.<br />
Secti<strong>on</strong> 3 Early Assessment and Diagnosis<br />
3.4 Investigati<strong>on</strong>s<br />
Once clinical diagnosis has been made, investigati<strong>on</strong>s<br />
are used to c<strong>on</strong>firm <strong>the</strong> diagnosis and to determine<br />
<strong>the</strong> potential cause of <strong>the</strong> event, specifically if <strong>the</strong>re is a<br />
cardiac or arterial source. Routine investigati<strong>on</strong>s<br />
should include full blood count, electrolytes, renal<br />
functi<strong>on</strong>, cholesterol and glucose levels and<br />
electrocardiogram although direct evidence is lacking<br />
<str<strong>on</strong>g>for</str<strong>on</strong>g> each of <strong>the</strong>se investigati<strong>on</strong>s. If clinical history,<br />
imaging and routine investigati<strong>on</strong>s do not adequately<br />
diagnose <strong>the</strong> underlying cause <strong>the</strong>n fur<strong>the</strong>r<br />
investigati<strong>on</strong>s may be warranted. Many tests exist<br />
and need to be c<strong>on</strong>sidered based <strong>on</strong> individual patient<br />
needs. For example, thrombophilia screening may<br />
be needed when <strong>the</strong> clinical history identifies a family<br />
history of thrombosis (particularly <str<strong>on</strong>g>for</str<strong>on</strong>g> those













