

Clinical Guidelines for Acute Stroke Management - Living on the EDge
Clinical Guidelines for Acute Stroke Management - Living on the EDge
Clinical Guidelines for Acute Stroke Management - Living on the EDge

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Secti<strong>on</strong> 5 Assessment and <str<strong>on</strong>g>Management</str<strong>on</strong>g> of <strong>the</strong> C<strong>on</strong>sequences of <str<strong>on</strong>g>Stroke</str<strong>on</strong>g><br />
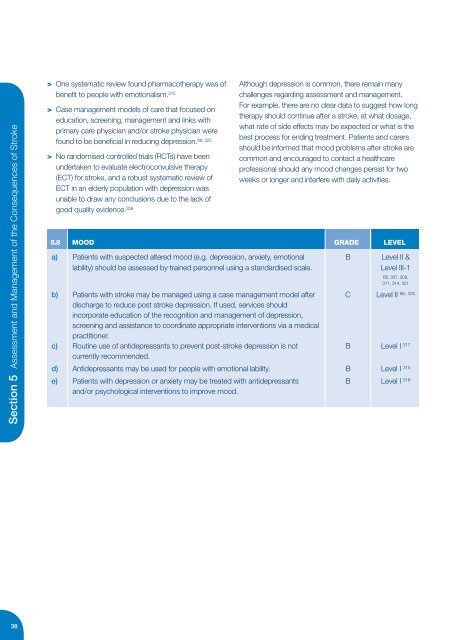
> One systematic review found pharmaco<strong>the</strong>rapy was of<br />
benefit to people with emoti<strong>on</strong>alism. 315<br />
> Case management models of care that focused <strong>on</strong><br />
educati<strong>on</strong>, screening, management and links with<br />
primary care physician and/or stroke physician were<br />
found to be beneficial in reducing depressi<strong>on</strong>.<br />
68, 325<br />
> No randomised c<strong>on</strong>trolled trials (RCTs) have been<br />
undertaken to evaluate electroc<strong>on</strong>vulsive <strong>the</strong>rapy<br />
(ECT) <str<strong>on</strong>g>for</str<strong>on</strong>g> stroke, and a robust systematic review of<br />
ECT in an elderly populati<strong>on</strong> with depressi<strong>on</strong> was<br />
unable to draw any c<strong>on</strong>clusi<strong>on</strong>s due to <strong>the</strong> lack of<br />
good quality evidence. 326<br />
Although depressi<strong>on</strong> is comm<strong>on</strong>, <strong>the</strong>re remain many<br />
challenges regarding assessment and management.<br />
For example, <strong>the</strong>re are no clear data to suggest how l<strong>on</strong>g<br />
<strong>the</strong>rapy should c<strong>on</strong>tinue after a stroke, at what dosage,<br />
what rate of side effects may be expected or what is <strong>the</strong><br />
best process <str<strong>on</strong>g>for</str<strong>on</strong>g> ending treatment. Patients and carers<br />
should be in<str<strong>on</strong>g>for</str<strong>on</strong>g>med that mood problems after stroke are<br />
comm<strong>on</strong> and encouraged to c<strong>on</strong>tact a healthcare<br />
professi<strong>on</strong>al should any mood changes persist <str<strong>on</strong>g>for</str<strong>on</strong>g> two<br />
weeks or l<strong>on</strong>ger and interfere with daily activities.<br />
5.8 MOOD GRADE LEVEL<br />
a) Patients with suspected altered mood (e.g. depressi<strong>on</strong>, anxiety, emoti<strong>on</strong>al B Level II &<br />
lability) should be assessed by trained pers<strong>on</strong>nel using a standardised scale.<br />
Level III-1<br />
68, 307, 309,<br />
311, 314, 321<br />
b) Patients with stroke may be managed using a case management model after C Level II<br />
68, 325<br />
discharge to reduce post stroke depressi<strong>on</strong>. If used, services should<br />
incorporate educati<strong>on</strong> of <strong>the</strong> recogniti<strong>on</strong> and management of depressi<strong>on</strong>,<br />
screening and assistance to coordinate appropriate interventi<strong>on</strong>s via a medical<br />
practiti<strong>on</strong>er.<br />
c) Routine use of antidepressants to prevent post-stroke depressi<strong>on</strong> is not B Level I 317<br />
currently recommended.<br />
d) Antidepressants may be used <str<strong>on</strong>g>for</str<strong>on</strong>g> people with emoti<strong>on</strong>al lability. B Level I 315<br />
e) Patients with depressi<strong>on</strong> or anxiety may be treated with antidepressants B Level I 316<br />
and/or psychological interventi<strong>on</strong>s to improve mood.<br />
38













