Gender in niGeria report 2012 - Economic Commission for Africa
Gender in niGeria report 2012 - Economic Commission for Africa
Gender in niGeria report 2012 - Economic Commission for Africa

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
44 <strong>Gender</strong> <strong>in</strong> Nigeria Report <strong>2012</strong>: Improv<strong>in</strong>g the Lives of Girls and Women <strong>in</strong> Nigeria<br />
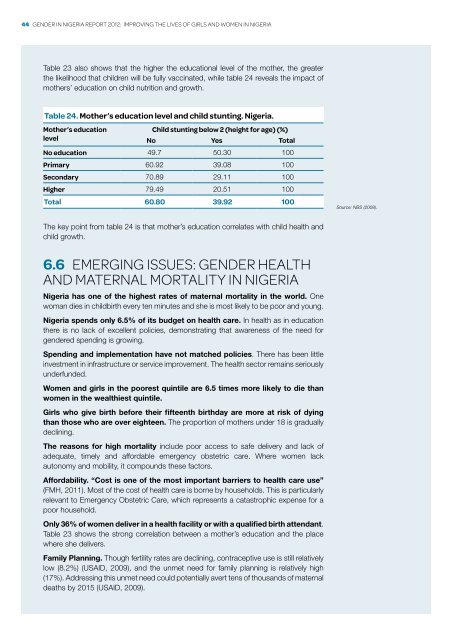
Table 23 also shows that the higher the educational level of the mother, the greater<br />
the likelihood that children will be fully vacc<strong>in</strong>ated, while table 24 reveals the impact of<br />
mothers’ education on child nutrition and growth.<br />
Table 24. Mother’s education level and child stunt<strong>in</strong>g. Nigeria.<br />
Mother’s education<br />
Child stunt<strong>in</strong>g below 2 (height <strong>for</strong> age) (%)<br />
level<br />
No Yes Total<br />
No education 49.7 50.30 100<br />
Primary 60.92 39.08 100<br />
Secondary 70.89 29.11 100<br />
Higher 79.49 20.51 100<br />
Total 60.80 39.92 100<br />
Source: NBS (2008).<br />
The key po<strong>in</strong>t from table 24 is that mother’s education correlates with child health and<br />
child growth.<br />
6.6 Emerg<strong>in</strong>g issues: gender health<br />
and maternal mortality <strong>in</strong> Nigeria<br />
Nigeria has one of the highest rates of maternal mortality <strong>in</strong> the world. One<br />
woman dies <strong>in</strong> childbirth every ten m<strong>in</strong>utes and she is most likely to be poor and young.<br />
Nigeria spends only 6.5% of its budget on health care. In health as <strong>in</strong> education<br />
there is no lack of excellent policies, demonstrat<strong>in</strong>g that awareness of the need <strong>for</strong><br />
gendered spend<strong>in</strong>g is grow<strong>in</strong>g.<br />
Spend<strong>in</strong>g and implementation have not matched policies. There has been little<br />
<strong>in</strong>vestment <strong>in</strong> <strong>in</strong>frastructure or service improvement. The health sector rema<strong>in</strong>s seriously<br />
underfunded.<br />
Women and girls <strong>in</strong> the poorest qu<strong>in</strong>tile are 6.5 times more likely to die than<br />
women <strong>in</strong> the wealthiest qu<strong>in</strong>tile.<br />
Girls who give birth be<strong>for</strong>e their fifteenth birthday are more at risk of dy<strong>in</strong>g<br />
than those who are over eighteen. The proportion of mothers under 18 is gradually<br />
decl<strong>in</strong><strong>in</strong>g.<br />
The reasons <strong>for</strong> high mortality <strong>in</strong>clude poor access to safe delivery and lack of<br />
adequate, timely and af<strong>for</strong>dable emergency obstetric care. Where women lack<br />
autonomy and mobility, it compounds these factors.<br />
Af<strong>for</strong>dability. “Cost is one of the most important barriers to health care use”<br />
(FMH, 2011). Most of the cost of health care is borne by households. This is particularly<br />
relevant to Emergency Obstetric Care, which represents a catastrophic expense <strong>for</strong> a<br />
poor household.<br />
Only 36% of women deliver <strong>in</strong> a health facility or with a qualified birth attendant.<br />
Table 23 shows the strong correlation between a mother’s education and the place<br />
where she delivers.<br />
Family Plann<strong>in</strong>g. Though fertility rates are decl<strong>in</strong><strong>in</strong>g, contraceptive use is still relatively<br />
low (8.2%) (USAID, 2009), and the unmet need <strong>for</strong> family plann<strong>in</strong>g is relatively high<br />
(17%). Address<strong>in</strong>g this unmet need could potentially avert tens of thousands of maternal<br />
deaths by 2015 (USAID, 2009).