

CPG for Psychosocial Interventions in Severe Mental ... - GuÃaSalud
CPG for Psychosocial Interventions in Severe Mental ... - GuÃaSalud
CPG for Psychosocial Interventions in Severe Mental ... - GuÃaSalud

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
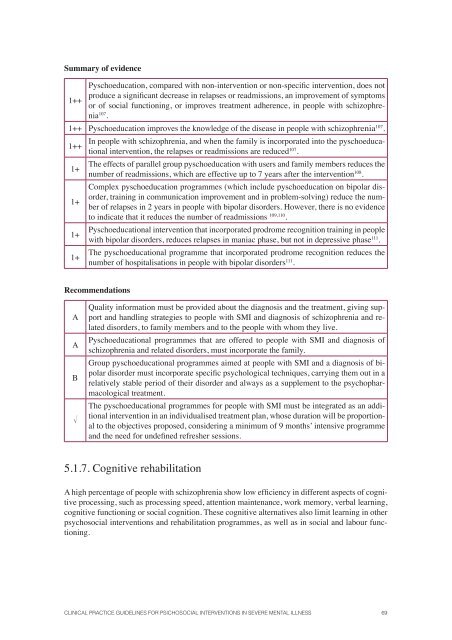
Summary of evidence<br />
Pyschoeducation, compared with non-<strong>in</strong>tervention or non-specific <strong>in</strong>tervention, does not<br />
produce a significant decrease <strong>in</strong> relapses or readmissions, an improvement of symptoms<br />
1++<br />
or of social function<strong>in</strong>g, or improves treatment adherence, <strong>in</strong> people with schizophrenia<br />
107 .<br />
1++ Pyschoeducation improves the knowledge of the disease <strong>in</strong> people with schizophrenia 107 .<br />
1++<br />
1+<br />
1+<br />
1+<br />
1+<br />
In people with schizophrenia, and when the family is <strong>in</strong>corporated <strong>in</strong>to the pyschoeducational<br />
<strong>in</strong>tervention, the relapses or readmissions are reduced 107 .<br />
The effects of parallel group pyschoeducation with users and family members reduces the<br />
number of readmissions, which are effective up to 7 years after the <strong>in</strong>tervention 108 .<br />
Complex pyschoeducation programmes (which <strong>in</strong>clude pyschoeducation on bipolar disorder,<br />
tra<strong>in</strong><strong>in</strong>g <strong>in</strong> communication improvement and <strong>in</strong> problem-solv<strong>in</strong>g) reduce the number<br />
of relapses <strong>in</strong> 2 years <strong>in</strong> people with bipolar disorders. However, there is no evidence<br />
to <strong>in</strong>dicate that it reduces the number of readmissions 109,110 .<br />
Pyschoeducational <strong>in</strong>tervention that <strong>in</strong>corporated prodrome recognition tra<strong>in</strong><strong>in</strong>g <strong>in</strong> people<br />
with bipolar disorders, reduces relapses <strong>in</strong> maniac phase, but not <strong>in</strong> depressive phase 111 .<br />
The pyschoeducational programme that <strong>in</strong>corporated prodrome recognition reduces the<br />
number of hospitalisations <strong>in</strong> people with bipolar disorders 111 .<br />
Recommendations<br />
A<br />
A<br />
B<br />
<br />
Quality <strong>in</strong><strong>for</strong>mation must be provided about the diagnosis and the treatment, giv<strong>in</strong>g support<br />
and handl<strong>in</strong>g strategies to people with SMI and diagnosis of schizophrenia and related<br />
disorders, to family members and to the people with whom they live.<br />
Pyschoeducational programmes that are offered to people with SMI and diagnosis of<br />
schizophrenia and related disorders, must <strong>in</strong>corporate the family.<br />
Group pyschoeducational programmes aimed at people with SMI and a diagnosis of bipolar<br />
disorder must <strong>in</strong>corporate specific psychological techniques, carry<strong>in</strong>g them out <strong>in</strong> a<br />
relatively stable period of their disorder and always as a supplement to the psychopharmacological<br />
treatment.<br />
The pyschoeducational programmes <strong>for</strong> people with SMI must be <strong>in</strong>tegrated as an additional<br />
<strong>in</strong>tervention <strong>in</strong> an <strong>in</strong>dividualised treatment plan, whose duration will be proportional<br />
to the objectives proposed, consider<strong>in</strong>g a m<strong>in</strong>imum of 9 months’ <strong>in</strong>tensive programme<br />
and the need <strong>for</strong> undef<strong>in</strong>ed refresher sessions.<br />
5.1.7. Cognitive rehabilitation<br />
A high percentage of people with schizophrenia show low efficiency <strong>in</strong> different aspects of cognitive<br />
process<strong>in</strong>g, such as process<strong>in</strong>g speed, attention ma<strong>in</strong>tenance, work memory, verbal learn<strong>in</strong>g,<br />
cognitive function<strong>in</strong>g or social cognition. These cognitive alternatives also limit learn<strong>in</strong>g <strong>in</strong> other<br />
psychosocial <strong>in</strong>terventions and rehabilitation programmes, as well as <strong>in</strong> social and labour function<strong>in</strong>g.<br />
CLINICAL PRACTICE GUIDELINES FOR PSICHOSOCIAL INTERVENTIONS IN SEVERE MENTAL ILLNESS 69














