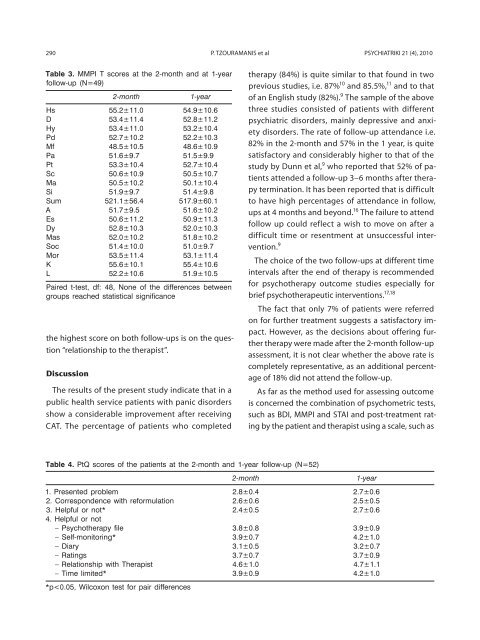
290 P. TZOURAMANIS et al PSYCHIATRIKI 21 (4), 2010Table 3. MMPI T scores at the 2-month and at 1-yearfollow-up (N=49)the highest score on both follow-ups is on the question“relationship to the therapist”.Discussion2-month1-yearHs 55.2±11.0 54.9±10.6D 53.4±11.4 52.8±11.2Hy 53.4±11.0 53.2±10.4Pd 52.7±10.2 52.2±10.3Mf 48.5±10.5 48.6±10.9Pa 51.6±9.7 51.5±9.9Pt 53.3±10.4 52.7±10.4Sc 50.6±10.9 50.5±10.7Ma 50.5±10.2 50.1±10.4Si 51.9±9.7 51.4±9.8Sum 521.1±56.4 517.9±60.1A 51.7±9.5 51.6±10.2Es 50.6±11.2 50.9±11.3Dy 52.8±10.3 52.0±10.3Mas 52.0±10.2 51.8±10.2Soc 51.4±10.0 51.0±9.7Mor 53.5±11.4 53.1±11.4K 55.6±10.1 55.4±10.6L 52.2±10.6 51.9±10.5Paired t-test, df: 48, None of the differences betweengroups reached statistical significanceThe results of the present study indicate that in apublic health service patients with panic disordersshow a considerable improvement after receivingCAT. The percentage of patients who completedtherapy (84%) is quite similar to that found in twoprevious studies, i.e. 87% 10 and 85.5%, 11 and to thatof an English study (82%). 9 The sample of the abovethree studies consisted of patients with differentpsychiatric disorders, mainly depressive and anxietydisorders. The rate of follow-up attendance i.e.82% in the 2-month and 57% in the 1 year, is quitesatisfactory and considerably higher to that of thestudy by Dunn et al, 9 who reported that 52% of patientsattended a follow-up 3–6 months after therapytermination. It has been reported that is difficultto have high percentages of attendance in follow,ups at 4 months and beyond. 16 The failure to attendfollow up could reflect a wish to move on after adifficult time or resentment at unsuccessful intervention.9The choice of the two follow-ups at different timeintervals after the end of therapy is recommendedfor psychotherapy outcome studies especially forbrief psychotherapeutic interventions. 17,18The fact that only 7% of patients were referredon for further treatment suggests a satisfactory impact.However, as the decisions about offering furthertherapy were made after the 2-month follow-upassessment, it is not clear whether the above rate iscompletely representative, as an additional percentageof 18% did not attend the follow-up.As far as the method used for assessing outcomeis concerned the combination of psychometric tests,such as BDI, MMPI and STAI and post-treatment ratingby the patient and therapist using a scale, such asTable 4. PtQ scores of the patients at the 2-month and 1-year follow-up (N=52)2-month1-year1. Presented problem 2.8±0.4 2.7±0.62. Correspondence with reformulation 2.6±0.6 2.5±0.53. Helpful or not* 2.4±0.5 2.7±0.64. Helpful or not– psychotherapy file 3.8±0.8 3.9±0.9– self-monitoring* 3.9±0.7 4.2±1.0– Diary 3.1±0.5 3.2±0.7– Ratings 3.7±0.7 3.7±0.9– Relationship with Therapist 4.6±1.0 4.7±1.1– Time limited* 3.9±0.9 4.2±1.0*p
PSYCHIATRIKI 21 (4), 2010 EVALUATION OF COGNITIVE-ANALYTIC THERAPY IN PANIC DISORDER 291PtQ, is considered to be the most appropriate. 19 Theuse of the above specific psychometric tests, whichare popular and reliable instruments, makes the assessmentapproach valid. On the other hand the factthat PtQ allows the patient to quantify helpful factorsof therapy is an excellent method for assessingtherapeutic outcome. 18,20According to the results of the tests, i.e. BDI, STAI,MMPI, the patients showed a considerable improvementat the 2-month follow-up comparedto pre-therapy evaluation. More important is thatthis improvement has been sustained at the 1-yearfollow-up. Especially, concerning MMPI the improvementwas measured by the 2 correspondinganxiety scales of the MMPI, i.e. A, Mas, in congruencewith other studies. 21 Also, a notable changeappeared on scale Dy (Dependence) and Es (Egostrength). The latter scale is the best index of a positivechange after treatment 22 and is usually incorporatedas a measure into psychotherapy outcomestudies. 19 Higher score after therapy means that theindividual tends to be better psychologically adjustedand that he/she is more capable to cope withproblems and stresses in life. 22 Furthermore, somepatients, apart from a panic disorder, received anadditional diagnosis of depressive disorders, whomdepressive symptomatolgy has also been ameliorated,as it seen in D corresponding clinical scaleand at BDI scores. Scale K of the MMPI is a validityscale measuring defensiveness but, in contrastto the other validity scale L of the test, it measuresmore subtle and mature defenses. 22 A higher scoreafter psychotherapy –if this score does not exceed60 for individuals of lower middle class and upperlower class, 22 as in the present study– is indicativeof improvement reflecting better functioning, egostrength and psychological resources. 22 It is worthwhileto mention that the other validity scale (L)did not manifest significant differences betweenthe pre and post-therapy assessment. It is also significantto refer that more than half of our patientshad a concomitant personality disorder. Therefore,CAT may have benefited them not only concerningpanic disorder, but mainly on personality. Theresults of the MMPl are validated by the results ofthe PtQ, where patients considered the new understandingmore helpful, as well as the fact that therapywas time limited at the time of 1-year follow,up than at the 2-month follow-up, when probablysome themes regarding separation had not beencompletely resolved.In conclusion, the present study indicated thatCAT is an effective therapeutic approach for patientswith PD. The above findings are importantespecially nowadays that pharmacotherapy is consideredto be the first choice of treatment for thesepatients. However, there are reports claiming thebeneficial effect of psychotherapeutic interventions.For instance, in a recent meta-analysis of 124 studies,Mitte 23 supported that CBT was at least as effectiveas pharmacotherapy and, depending on the type ofanalysis, even significantly more effective. In addition,CAT treats PD in a short time while simultaneouslyinflicting beneficial changes to the personalitystructure, thus reducing the possibility of recurrence.It is worthwhile to note that more than half of thepatients of the present study had an additional diagnosisof a personality disorder. Finally, another advantagecould be the avoidance of the side effects ofthe drugs.
- Page 5: PSYCHIATRIKIQuarterly journal publi
- Page 9 and 10: PSYCHIATRIKI 21 (4), 2010 277Άρθ
- Page 11 and 12: PSYCHIATRIKI 21 (4), 2010 279Resear
- Page 13 and 14: PSYCHIATRIKI 21 (4), 2010 HOSPITAL
- Page 15 and 16: PSYCHIATRIKI 21 (4), 2010 HOSPITAL
- Page 17 and 18: PSYCHIATRIKI 21 (4), 2010 HOSPITAL
- Page 19 and 20: PSYCHIATRIKI 21 (4), 2010 287Resear
- Page 24 and 25: 292 P. TZOURAMANIS et al PSYCHIATRI
- Page 26 and 27: 294 PSYCHIATRIKI 21 (4), 2010Resear
- Page 28 and 29: 296 M. VLASSOPOULOS et al PSYCHIATR
- Page 30 and 31: 298 M. VLASSOPOULOS et al PSYCHIATR
- Page 32 and 33: 300 M. VLASSOPOULOS et al PSYCHIATR
- Page 34 and 35: 302 M. VLASSOPOULOS et al PSYCHIATR
- Page 36 and 37: 304 PSYCHIATRIKI 21 (4), 2010Resear
- Page 38 and 39: 306 H. LAZARATOU et al PSYCHIATRIKI
- Page 40 and 41: 308 H. LAZARATOU et al PSYCHIATRIKI
- Page 42 and 43: 310 H. LAZARATOU et al PSYCHIATRIKI
- Page 44 and 45: 312 H. LAZARATOU et al PSYCHIATRIKI
- Page 46 and 47: 314 H. LAZARATOU et al PSYCHIATRIKI
- Page 48 and 49: 316 C. Kouimtsidis PSYCHIATRIKI 21
- Page 50 and 51: 318 C. Kouimtsidis PSYCHIATRIKI 21
- Page 52 and 53: 320 C. Kouimtsidis PSYCHIATRIKI 21
- Page 54 and 55: 322 C. Kouimtsidis PSYCHIATRIKI 21
- Page 56 and 57: 324 PSYCHIATRIKI 21 (4), 2010Specia
- Page 58 and 59: 326 B.J. HAVAKI-KONTAXAKI et al PSY
- Page 60 and 61: 328 B.J. HAVAKI-KONTAXAKI et al PSY
- Page 62 and 63: 330 B.J. HAVAKI-KONTAXAKI et al PSY
- Page 64 and 65: 332 PSYCHIATRIKI 21 (4), 2010Genera
- Page 66 and 67: 334 C.I. Istokoglou et al PSYCHIATR
- Page 68 and 69: 336 C.I. Istokoglou et al PSYCHIATR
- Page 70 and 71: 338 C.I. Istokoglou et al PSYCHIATR
- Page 72 and 73:
340 PSYCHIATRIKI 21 (4), 2010• 10
- Page 74 and 75:
SUBMISSIONPapers either in English
- Page 76 and 77:
ΥΠΟΒΟΛΗ ΕΡΓΑΣΙΩΝΟι
- Page 78:
ΣΥΝΟΔΕΥΤΙΚΟ ΕΝΤΥΠΟ