<strong>June</strong> <strong>2007</strong>KUWAIT MEDICAL JOURNAL 121Cigarette smoking is the nations’ leading causeof premature mortality, and is responsible for onethirdof all deaths among working - age Americans.Smoking cigarettes is both psychologically andphysiologically addictive. Careless smoking alsocan cause severe burn injuries and death. Many ofthe adverse effects of smoking occur in secondhand(passive) smokers [10] .Twenty-three percent of adults aged 18 years orolder smoke cigarettes. Over 400,000 adults diefrom tobacco-related diseases each year [11] . Smokingaffects not only the tobacco user but also those nearthe smoker, such as family, friends, co-workers andunborn children. A p p roximately 24 billion packagesof cigarettes are purchased annually. In <strong>June</strong> 2002,the International Agency for Research on Cancerconcluded that involuntary smoking (exposure tosecondhand or “environmental” tobacco smoke)was carcinogenic to humans [12] . National expendituresattributable to cigarette smoking surpass $ 75billion in medical costs plus $80 billion in indirectcosts [13] .The Food and Agricultural Organization of theUnited Nations (FAO) estimated that tobaccoconsumption in developing nations was increasingat a rate of 1.9 percent during 1995 - 2000 [14] . One ofthe reasons which explain this rise is lack ofawareness of health risks associated with tobaccouse, particularly the fact that there is approximatelya 25 - 30 year lag time between the onset ofpersistent tobacco use and the actual deathsattributable to smoking.S m o k i n g - related diseases re p resent an enormouseconomic burden on the health care system. Inaddition to the traditional burden of communicablediseases, developing countries today are faced witha huge increase in non-communicable diseases,mental illness and violence and injuries. Smokingcosts the national health services (NHS) approximately$ 1.5 billion a year for treating diseasescaused by smoking. This includes the cost ofhospital admissions, general practitionerconsultations and prescriptions. In 1997-98, 364,200people were admitted to NHS hospitals to betreated for diseases related to smoking. On anaverage, they occupy 9,500 hospitals bed per yearevery day [15] .In Kuwait, smoking prevalence among adultmales (18 - 60 yrs) was 34.4% in 1998 [16] whilesmoking prevalence among youth (10 -18yrs) wasreported as 23.1% [ 17 ] . Our survey was done toestimate the prevalence of smoking in Kuwait andits economic cost on the health care system.SUBJECTS AND METHODSWe conducted a cross-sectional survey amongpersons seeking medical care at Al-Saqer specializedhealth center (which served Al-Adeiyliyah and Al-Faiha areas) and Al-Yarmok primary health center(which served A l - Yarmok and Qurtoba are a s ) .These were selected as the setting for our study. Wedecided to enroll all male Kuwaiti and non Kuwaitipersons ∆ 18 years coming to these health centers.The survey collected information on socioeconomiccharacteristics (age, marital status, levelof education, employment and nationality),p resence of some chronic diseases such ashypertension, diabetes, cardiovascular diseases,chronic pulmonary diseases, bronchial asthma andsmoking status.Respondents were classified as current smoker,former smoker and never smoker.A current smokerwas defined as anyone who had smoked more than100 cigarettes in his lifetime and continued tosmoke at least one cigarette daily. A former-smokerwas one who had smoked more than 100 cigarettesin his lifetime but no longer smoked. A neversmokerwas one who had never smoked or hadsmoked fewer than 100 cigarettes in his lifetime [18] .Current smokers were asked about onset of regularsmoking, kind of smoking, the number ofcigarettes.All respondents were asked about: reason forhealth center visit, date of last visit to health centeror hospital and the reasons for those visits. We alsocollected data about number of visits to privateclinics as well as pharmacies seeking medical careduring last six months.Data were collected through January - February2003. The number of cases collected during thisperiod was deemed to be enough for analysis(consensus sample). The questionnaire was pilottested on a random sample of one hundred personsand some of the questions were modified before itwas formally used. For the sample, one hundredq u e s t i o n n a i res were distributed and self administere dand a team of trained doctors interviewed Kuwaitiand non-Kuwaiti males age > 18 yrs. The responserate was 100%.In the actual study, two thousand two hundredand sixteen males were interviewed by trainedphysicians and respondents were told that theinformation obtained would be confidential andused only for statistical purposes to minimize nonresponseand under-reporting.Case definition for the illnesses presented bypatients: patients were classified according todiagnosis code of international classification ofdiseases (ICD-10-CM) after confirming the diagnosisfrom the attending physician (Table 1).Data was analyzed using SPSS statisticalp rogram and descriptive statistics includingfrequencies, mean and standard deviation wereused to describe the study findings. The association
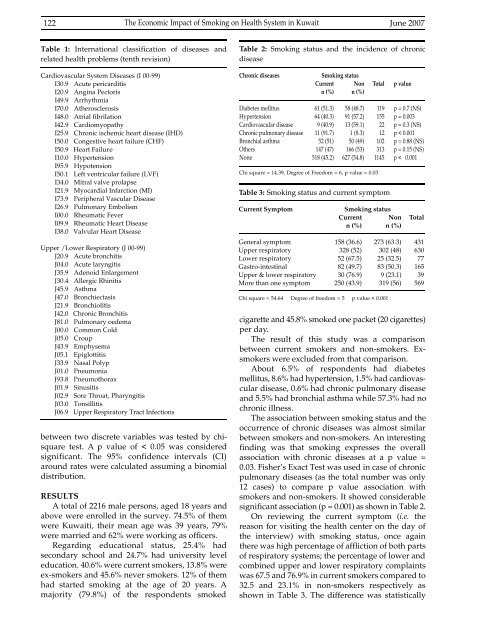
122The Economic Impact of Smoking on Health System in Kuwait <strong>June</strong> <strong>2007</strong>Table 1: International classification of diseases andrelated health problems (tenth revision)Cardiovascular System Diseases (I 00-99)I30.9 Acute pericarditisI20.9 Angina PectorisI49.9 ArrhythmiaI70.0 AtherosclerosisI48.0 Atrial fibrilationI42.9 CardiomyopathyI25.9 Chronic ischemic heart disease (IHD)I50.0 Congestive heart failure (CHF)I50.9 Heart FailureI10.0 HypertensionI95.9 HypotensionI50.1 Left ventricular failure (LVF)I34.0 Mitral valve prolapseI21.9 Myocardial Infarction (MI)I73.9 Peripheral Vascular DiseaseI26.9 Pulmonary EmbolismI00.0 Rheumatic FeverI09.9 Rheumatic Heart DiseaseI38.0 Valvular Heart DiseaseUpper /Lower Respiratory (J 00-99)J20.9 Acute bronchitisJ04.0 Acute laryngitisJ35.9 Adenoid EnlargementJ30.4 Allergic RhinitisJ45.9 AsthmaJ47.0 BronchiectasisJ21.9 BronchiolitisJ42.0 Chronic BronchitisJ81.0 Pulmonary oedemaJ00.0 Common ColdJ05.0 CroupJ43.9 EmphysemaJ05.1 EpiglottitisJ33.9 Nasal PolypJ01.0 PneumoniaJ93.8 PneumothoraxJ01.9 SinusitisJ02.9 Sore Throat, PharyngitisJ03.0 TonsillitisJ06.9 Upper Respiratory Tract Infectionsbetween two discrete variables was tested by chisquaretest. A p value of < 0.05 was consideredsignificant. The 95% confidence intervals (CI)around rates were calculated assuming a binomialdistribution.RESULTSA total of 2216 male persons, aged 18 years andabove were enrolled in the survey. 74.5% of themwere Kuwaiti, their mean age was <strong>39</strong> years, 79%were married and 62% were working as officers.R e g a rding educational status, 25.4% hadsecondary school and 24.7% had university leveleducation. 40.6% were current smokers, 13.8% wereex-smokers and 45.6% never smokers. 12% of themhad started smoking at the age of 20 years. Amajority (79.8%) of the respondents smokedTable 2: Smoking status and the incidence of chronicdiseaseChronic diseasesSmoking statusCurrent Non Total p valuen (%) n (%)Diabetes mellitus 61 (51.3) 58 (48.7) 119 p = 0.7 (NS)Hypertension 64 (40.3) 91 (57.2) 155 p = 0.003Cardiovascular disease 9 (40.9) 13 (59.1) 22 p = 0.3 (NS)Chronic pulmonary disease 11 (91.7) 1 (8.3) 12 p < 0.001Bronchial asthma 52 (51) 50 (49) 102 p = 0.88 (NS)Others 147 (47) 166 (53) 313 p = 0.15 (NS)None 518 (45.2) 627 (54.8) 1145 p < 0.001Chi square = 14.<strong>39</strong>, Degree of Freedom = 6, p value = 0.03Table 3: Smoking status and current symptomCurrent SymptomSmoking statusCurrent Non Totaln (%) n (%)General symptom 158 (36.6) 273 (63.3) 431Upper respiratory 328 (52) 302 (48) 630Lower respiratory 52 (67.5) 25 (32.5) 77Gastro-intestinal 82 (49.7) 83 (50.3) 165Upper & lower respiratory 30 (76.9) 9 (23.1) <strong>39</strong>More than one symptom 250 (43.9) 319 (56) 569Chi square = 54.64 Degree of freedom = 5 p value < 0.001 :c i g a rette and 45.8% smoked one packet (20 cigare t t e s )per day.The result of this study was a comparisonbetween current smokers and non-smokers. Exsmokerswere excluded from that comparison.About 6.5% of respondents had diabetesmellitus, 8.6% had hypertension, 1.5% had card i o v a s -cular disease, 0.6% had chronic pulmonary diseaseand 5.5% had bronchial asthma while 57.3% had nochronic illness.The association between smoking status and theoccurrence of chronic diseases was almost similarbetween smokers and non-smokers. An interestingfinding was that smoking expresses the overallassociation with chronic diseases at a p value =0.03. Fisher’s Exact Test was used in case of chronicpulmonary diseases (as the total number was only12 cases) to compare p value association withsmokers and non-smokers. It showed considerablesignificant association (p = 0.001) as shown in Table 2.On reviewing the current symptom (i.e. thereason for visiting the health center on the day ofthe interview) with smoking status, once againthere was high percentage of affliction of both partsof respiratory systems; the percentage of lower andcombined upper and lower respiratory complaintswas 67.5 and 76.9% in current smokers compared to32.5 and 23.1% in non-smokers respectively asshown in Table 3. The difference was statistically