

Chapter 96

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Thoracic Surgery:<br />
Surgical Considerations<br />
<strong>96</strong><br />
J. Ted Gerstle CHAPTER<br />
INTRODUCTION<br />
The topic of pediatric thoracic surgery is large and constantly<br />
changing. This change is being driven in part by issues including:<br />
(1) the increasing use of antenatal ultrasounds with the subsequent<br />
identification of lung lesions, which previously may have remained<br />
quiescent, asymptomatic, and thus, undiagnosed; (2) higher-quality<br />
diagnostic imaging studies, which have the ability to identify<br />
smaller and smaller abnormalities in the lung; and (3) the<br />
increasing use of minimal access surgical techniques in the chest,<br />
both diagnostically and therapeutically. The latter has been gaining<br />
great momentum as surgical skills have matured and operative<br />
equipment has improved, including the adaptation of this<br />
equipment to the smaller body habitus of a child. This chapter on<br />
pediatric thoracic surgery will emphasize the role of thoracoscopy<br />
and highlight some of the new indications for its use. Where<br />
possible, data will be presented in an evidence-based fashion. The<br />
format of individual thoracic diseases and abnormalities will<br />
include (where it is indicated and it gives clarity to the discussion<br />
of the topic): (1) clinical presentation, (2) diagnostic moda -<br />
lities, (3) preoperative considerations, (4) intraoperative consi -<br />
derations, and (5) postoperative considerations. Purposefully,<br />
certain topics will be excluded from discussion in this chapter,<br />
because they will be reviewed in other chapters of this textbook,<br />
including esophageal atresia, tracheoesophageal fistula, congenital<br />
diaphragmatic hernia (neonatal), tracheomalacia and tracheal<br />
stenosis.<br />
NEOPLASMS<br />
The use of thoracoscopic procedures in children has been<br />
broadened to include its use in the diagnosis and treatment<br />
of neoplasms. The size of solid malignancies and benign tumors<br />
in children limits the use of therapeutic thoracoscopy. Therefore,<br />
minimally invasive diagnostic procedures are more common<br />
in children than therapeutic procedures for malignancy.<br />
Current diagnostic and therapeutic thoracoscopic procedures<br />
discussed in this section include: (1) diagnostic thoracoscopy,<br />
(2) thoracoscopic lung biopsies, (3) thoracoscopic mediastinal<br />
biopsies, and (4) thoracoscopic tumor resections of the media -<br />
stinum.<br />
When considering the use of thoracoscopy for pediatric<br />
malignancies and tumors, the potential short-term and long-term<br />
benefits must be reviewed. The short-term benefits are similar to<br />
many procedures using thoracoscopy (e.g., less pain, shorter<br />
recovery period, etc.). With malignancies, however, it is the longterm<br />
benefits that are more important, specifically recurrence rates<br />
and survival. A significant amount of basic science has been<br />
carried out to investigate the role of minimal access surgery (MAS)<br />
and its potential to either positively or negatively alter the outcome<br />
of children with malignancies. 1–3<br />
Thoracic Lung Biopsy<br />
Waldhausen et al. published a study that reviewed their experience<br />
with MAS and clinical decision-making with pediatric<br />
cancer patients. 4 Video 1 demonstrates a right-sided computed<br />
tomography (CT)-guided lung tattooing in which two lesions in<br />
the superior lower lobe have been marked before a thoracoscopic<br />
lung biopsy. The investigators thought that the benefits of the<br />
thoracoscopic procedures were (1) alleviating the need for open<br />
thoracotomy and thus, avoiding the associated morbidity of<br />
this procedure, (2) hastening of the recovery time, and<br />
(3) improved visualization of the pleural surfaces. Limitations<br />
where thoracoscopy was not useful included (1) medial-located<br />
pulmonary lesions (where CT-guided needle localization could<br />
not be used), (2) children who had uncorrectable coagulopathies,<br />
and (3) children in whom an ipsilateral pneumothorax could<br />
not be created safely. Overall, thoracoscopy was felt to be accurate<br />
and safe.<br />
On the basis of this study and other studies, a few conclusions<br />
can be made 5–7 ; (1) thoracoscopic biopsies are accurate, have a low<br />
complication rate and appear to have a faster rate of recovery;<br />
(2) the initial approach to a pulmonary lesion may be with a<br />
percutaneous approach where the biopsy is for diagnostic<br />
purposes and the lesion is larger than 5 mm in diameter; and<br />
(3) in the case of a percutaneous biopsy, there is a relatively high<br />
chance that a second biopsy may have to be performed to obtain<br />
a definitive diagnosis. Although thoracoscopy is effective for<br />
diagnostic purposes, its role in the therapeutic realm remains<br />
untested. Presently, there is no role for thoracoscopic surgery in<br />
the treatment of children requiring pulmonary resections for<br />
multiple metastatic lesions, including osteogenic sarcoma and<br />
peripheral nerve sheath tumors. In these tumors, it is imperative<br />
that all palpable lesions be removed. There is no means to locate<br />
these lesions such that thoracoscopy can be effective; they are<br />
often missed on CT scan imaging 8 and only noted on direct<br />
palpation. As the precise excision of these metastatic lesions will<br />
directly influence the patient’s survival, they should always be<br />
addressed with a thoracotomy.
1642 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
Thoracoscopic Mediastinal Biopsies<br />
In the pediatric patients of various studies, thoracoscopic biopsy<br />
of mediastinal masses has been demonstrated to be safe and<br />
effective. 4,9 Thoracoscopic mediastinal biopsy is contraindicated,<br />
however, in children in whom carinal and subcarinal compression<br />
from the anterior mediastinal mass can be demonstrated. For<br />
these situations, percutaneous biopsy with local anesthesia only<br />
or 24 hours of intravenous steroids are recommended. 10–13<br />
Alternatively, a Chamberlain procedure in a semiupright position<br />
under local anesthesia, with spontaneous ventilation, can be<br />
helpful in patients in whom a needle diagnosis of Hodgkin disease<br />
(HD) is unable to be obtained. 12 A single case has been reported<br />
in which radiation was administered to a limited area of the tumor<br />
before the initial biopsy was performed. A diagnosis was<br />
established based on tissue from the shielded area after the main<br />
mass had decreased in size. 14 To minimize morbidity and mortality<br />
in those children undergoing a biopsy of a mediastinal mass the<br />
following have been recommended: a tracheal diameter of at least<br />
50% of normal and a peak expiratory flow rates of at least 50% of<br />
predicted value. 12 Deviation from these standards may result in<br />
loss of the airway or hemodynamic collapse while undergoing<br />
induction for a general anesthetic with subsequent mortality.<br />
Thoracoscopic Tumor Resections<br />
of the Mediastinum<br />
Thoracoscopic resection of mediastinal masses in children has<br />
been limited. There have been reports of resection of benign<br />
neurogenic tumors of the posterior mediastinum in adults and a<br />
few children. 15–16 In a more recent study by Lacreuse et al., the<br />
authors examined the role of thoracoscopy in the resection of<br />
posterior mediastinal tumors that were neurogenic in origin:<br />
ganglioneuroma, ganglioneuroblastoma, and neuroblastoma. 17<br />
The procedures had minimal complications, including two<br />
chylothoraces that improved with conservative management and<br />
one conversion to an open thoracotomy. The authors felt<br />
thoracoscopic resection is a feasible, safe, and efficient procedure,<br />
as it allows for improved visualization of the tumor and its<br />
anatomic connections and resection can be as complete as an open<br />
procedure without having to complicate the operative technique in<br />
the same operating time.<br />
Mediastinal Neoplasms<br />
In general, these malignancies are separated into groups on the<br />
basis of location within the mediastinum, including the anterior,<br />
middle, and posterior regions of the mediastinum; for purposes<br />
of this discussion, the superior region of the mediastinum is<br />
grouped with the anterior region (Table <strong>96</strong>–1). The relative<br />
incidence of the common mediastinal neoplasms is given in Table<br />
<strong>96</strong>–2. Although lymphangiomas are not mediastinal neoplasms<br />
per se, they have important clinical issues as masses in the<br />
mediastinum and will be discussed in this section.<br />
Hodgkin Disease<br />
Lymphoid tumors which include HD and non-Hodgkin<br />
lymphoma (NHL) account for the highest percentage of<br />
mediastinal masses in children. 18 The majority of patients with<br />
Hodgkin disease will be older than 17 years; 11% are 11 to 16 years<br />
and 4% are younger than 10 years. Children who are diagnosed at<br />
TABLE <strong>96</strong>-1. Different Types of Mediastinal Neoplasms,<br />
by Region Within the Mediastinum<br />
Anterior a Middle Posterior<br />
Thymoma Non-Hodgkin Ganglioneuroma<br />
lymphoma<br />
Thymic carcinoma Hodgkin Ganglioneuroblastoma<br />
lymphoma<br />
Non-Hodgkin Pericardial Neuroblastoma<br />
lymphoma<br />
teratoma<br />
Hodgkin lymphoma Cardiac rhab- Pheochromocytoma<br />
domyoma<br />
Teratoma Lipoblastoma PNET<br />
Germ cell tumor<br />
Lipoblastoma<br />
Lipoblastoma<br />
PNET = primitive neuroectodermal tumor.<br />
a<br />
Anterior includes the anterior and superior regions.<br />
an age of less than 16 years have the best prognosis. Clinically,<br />
cervical, mediastinal, axillary, and inguinal lymphadenopathy are<br />
noted in 80%, 50%, 33% and 5% of the patients, respectively; some<br />
children will also have symptoms of weight loss, fever, and night<br />
sweats, which portend a worse prognosis. The treatment of this<br />
disease is nonsurgical, consisting of chemotherapy and radiotherapy.<br />
The challenge posed to the surgical and anesthesia teams<br />
is how to safely obtain pathologic tissue to confirm the diagnosis<br />
and determine the histologic subtype of HD. As a high percentage<br />
of patients will have a concurrent mediastinal mass, the risk of a<br />
major intraoperative complication of cardiorespiratory collapse is<br />
potentially very high. To avert this risk, a series of preoperative<br />
tests can be performed: echocardiography, chest CT scan, and<br />
pulmonary function tests.<br />
Shamberger et al. used the cross-sectional area of the trachea on<br />
CT scan scanning to predict anesthetic complications and used it<br />
to determine who would be a candidate for local anesthesia versus<br />
general anesthesia. 19 Hack et al. found that a tracheal crosssectional<br />
area of
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1643<br />
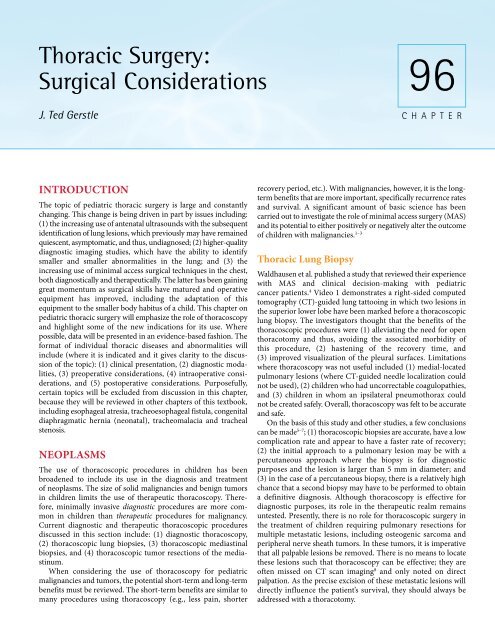
Figure <strong>96</strong>-1. Computed tomography scan (axial) of the chest of<br />
a patient with an anterior mediastinal mass related to Hodgkin<br />
disease. The mass is projecting in the left hemithorax and is<br />
shifting the mediastinal structures into the contralateral chest.<br />
In addition, there is extension of the mass into the soft tissues<br />
of the anterior chest and sternum.<br />
The most significant predictor of anesthetic complications appears<br />
to be a clinical finding of stridor and/or positional dyspnea; in<br />
these patients, general anesthesia should be avoided and a<br />
peripheral lymph node which can be biopsied under local anesthesia<br />
should be sought. 20–21<br />
Non-Hodgkin Lymphoma<br />
NHL is the third most common malignancy in childhood. There<br />
are three types of NHL that occur in children, making up >90% of<br />
diagnoses: lymphoblastic lymphoma, small–noncleaved-cell<br />
(Burkitt and non-Burkitt) lymphoma and large-cell lymphoma.<br />
Various immunodeficiency states are associated with NHL:<br />
human immunodeficiency virus, Wiskott-Aldrich syndrome,<br />
Bloom syndrome, ataxia telangiectasia, severe combined immunodeficiency<br />
disease, X-linked lymphoproliferative syndrome,<br />
and organ transplantation. Clinically, NHL presents abruptly and<br />
can progresses rapidly, having wide spread lymph node and<br />
extralymphoid involvement. Mediastinal involvement is predicted<br />
by the type of NHL with lymphoblastic lymphoma presenting<br />
most commonly in the anterior mediastinum in 50 to 75% of<br />
cases. In addition, some types of NHL, such as small–noncleavedcell<br />
(Burkitt’s and non-Burkitt’s) lymphoma, can have a tumor<br />
doubling time of 24 hours, making rapid diagnosis of paramount<br />
importance to avoid the complication of tumor lysis syndrome<br />
(hyperuricemia related to rapid cell death). The approach to the<br />
management of an anterior mediastinal mass in NHL is similar to<br />
HD; however, there are often other options to safely obtain a tissue<br />
diagnosis with NHL using local anesthesia which should be<br />
considered. These include bone marrow biopsy, aspiration of<br />
thoracic effusions, and aspiration of ascites.<br />
Neurogenic Tumors<br />
Neurogenic tumors, which include ganglioneuroma, ganglioneuroblastoma,<br />
and neuroblastoma, are the second most common<br />
mediastinal neoplasm in children; the vast majority of these<br />
are located in the posterior mediastinum. From a thoracic<br />
Figure <strong>96</strong>-2. Thoracoscopic view of a neuroblastoma arising<br />
from a stellate ganglion in the apex of the right hemithorax in a<br />
patient who presented with a Horner syndrome.<br />
presentation perspective, these children may present with respiratory<br />
distress or a Horner syndrome (ipsilateral ptosis, myosis,<br />
anhydrosis, and heterochromia). Figure <strong>96</strong>–2 demonstrates a<br />
thoracoscopic view of a neuroblastoma arising from a stellate<br />
ganglion in the right chest in a patient who presented with Horner<br />
syndrome; figure <strong>96</strong>–3 illustrates this same right-sided thoracic<br />
tumor on a coronal view of a magnetic resonance image. These<br />
patients may also present with neurologic symptoms related to a<br />
dumbbell-shaped tumor involving the chest and spinal canal<br />
simultaneously; the latter may have cauda equina syndrome or<br />
paraplegia. 23<br />
Figure <strong>96</strong>-3. Magnetic resonance image (coronal) of a patient<br />
with clinical features of a Horner syndrome and a right-sided<br />
thoracic tumor in the apex of the chest, likely arising from the<br />
ipsilateral stellate ganglion.
1644 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
A<br />
Figure <strong>96</strong>-4. Magnetic resonance image (axial) of a large rightthoracic<br />
neuroblastoma with extension into the spinal canal and<br />
compression of the cord. This patient presented with bilateral<br />
lower-extremity weakness.<br />
The diagnosis and treatment of these tumors is complex and is<br />
actively altered per international, multicenter clinical trials<br />
conducted by the Children’s Oncology Group. Prognosis is also<br />
complex and is based on the stage of the disease, the age of the<br />
patient (age
intrapericardial GCT and cardiac GCT. Intrapericardial GCT<br />
occurs most commonly in infants who are less than 12 months old<br />
and present with findings of cardiac tamponade and congestive<br />
heart failure; as most are benign, they are treated with primary<br />
resection. They can have a very complicated intraoperative course<br />
because they often compress the adjacent atria and ascending aorta.<br />
Cardiac GCTs, which are malignant in 25% of the cases, present<br />
with congestive heart failure and/or arrhythmias (as intraventricular<br />
block) and are most commonly located in the right side<br />
of the heart. They are associated with congenital heart disease<br />
(atrial and ventricular septal defects). Although primary surgical<br />
resection is indicated to avert complete cardiac outflow<br />
obstruction, there are times when the GCT is unresectable, making<br />
cardiac transplantation an option. 24<br />
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1645<br />
Lymphangioma<br />
Although these lesions are also referred to as cystic hygromas, the<br />
more current term is lymphangioma. They have an incidence of<br />
1 in 12,000 births and approximately 50 to 65% of them are present<br />
at birth; the vast majority becomes clinically evident before 2 years<br />
of life. 25 They develop as a result of the failure of primitive<br />
lymphatic buds to form communications with adjacent developing<br />
veins; these buds dilate into lymphatic cysts which subsequently<br />
become lymphangiomas. Anatomically, they are most commonly<br />
found in the neck (75%) and less commonly in the mediastinum<br />
(
1646 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
A<br />
B<br />
C<br />
Figure <strong>96</strong>-8. A and B: Intraoperative series demonstrates a posterior approach to resection of a superior, left-sided Ewing sarcoma<br />
of the chest wall. The muscles on the medial side of the scapula are divided and it is reflected laterally and superiorly. After the ribs<br />
are divided, that portion of the lung that is adherent to the chest wall tumor is divided with a stapler to deliver the chest wall, tumor,<br />
and lung en bloc. The remaining chest wall defect will be closed with Marlex mesh.<br />
D<br />
Ewing sarcoma; the muscles on the medially side of the scapula<br />
are divided and it is reflected laterally.<br />
Intraoperative considerations include one-lung ventilation and<br />
epidural catheter placement. The former allows confirmation of<br />
which ribs must be removed and facilitates the resection of<br />
contiguous structures as the adjacent lung which may or may not<br />
be adherent to the tumor; the latter provides good postoperative<br />
analgesia. With this careful planning and approach, large areas of<br />
chest wall can be safely resected in sections up to six ribs (and<br />
seven intercostal spaces) in height. 27 Figure <strong>96</strong>–9 shows a large<br />
Ewing sarcoma on the left chest wall after resection.<br />
Pulmonary Neoplasms<br />
Primary neoplasms of the lung in children, including bronchogenic<br />
carcinoma, bronchial carcinoid tumor, and pleuropulmonary<br />
blastoma, are extremely rare. 28 Metastatic disease to<br />
the lung is more common, and this entity will be briefly reviewed<br />
in this section. Many neoplasms may develop metastatic disease,<br />
including those listed in Table <strong>96</strong>–3. Osteogenic sarcoma, alveolar<br />
soft part sarcoma, and adrenocortical carcinoma are tumors which<br />
can result in pulmonary metastases and are associated with a more<br />
favorable clinical outcome with pulmonary metastasectomy; the<br />
other six tumors listed have unclear or no impact on clinical<br />
outcome. 29 When preoperatively assessing candidates for<br />
pulmonary metastasectomy, it is important to consider the<br />
number of lesions, the size of the lesions, whether the lesions are<br />
unilateral or bilateral, the proximity of the lesions to major bronchi<br />
and main pulmonary vessels, and the anticipated amount of lung<br />
that will need to be resected to obtain clear surgical margins (and<br />
the corollary: how much lung will remain). In addition, it is<br />
important to recognize and plan for resecting more pulmonary<br />
lesions than are identified on CT scan; this is particularly relevant<br />
with metastatic disease from osteogenic sarcoma, where one study<br />
has reported that more than half of the lesions that are ≤5 mm<br />
will be missed on CT scan. 8 Figure <strong>96</strong>–10 demonstrates a very<br />
small right-sided lung lesion that is typical of metastatic<br />
osteogenic sarcoma.
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1647<br />
Figure <strong>96</strong>-9. A large Ewing sarcoma on the left chest wall after<br />
resection. The ribs are oriented anterior to the mass as though<br />
the tumor were still in vivo.<br />
The surgical team must consider the surgical approach: (1)<br />
bilateral posteriolateral thoracotomies give optimal access to the<br />
lung in each hemithorax, but such approaches may be limited<br />
if a relatively large amount of lung parenchyma will need to be<br />
resected (in addition, such approaches make postoperative pain<br />
difficult); (2) median sternotomy gives access to both hemithoraces<br />
simultaneously and are associated with less postoperative<br />
pain, but it is difficult to assess and resect pulmonary lesions<br />
in the posterior portions of the lung with this approach; and (3)<br />
staged unilateral posteriolateral thoracotomies allow for optimal<br />
access to the lung in each hemithorax, are better if it is anticipated<br />
that a large amount of lung will need to be resected, but do<br />
require a second anesthetic. Usually, a 2-week hiatus between<br />
procedures allows the ipsilateral lung to recover from postoperative<br />
hemorrhage and edema before resection of parts of<br />
the contralateral lung. It is this author’s preference to optimize<br />
surgical exposure and resectability of these pulmonary lesions<br />
by using the latter approach for bilateral lung lesions. Preoperative<br />
pulmonary function tests (PFT) are required to assess changes<br />
in respiratory function between thoracotomies and may predict<br />
the need for postoperative critical care bed needs; in general, PFTs<br />
are not effective in predicting whether a patient will tolerate<br />
one-lung ventilation or not. Intraoperative considerations<br />
mandate that one-lung ventilation be established to allow optimal<br />
palpation of the entire lung and resect all metastatic lesions;<br />
TABLE <strong>96</strong>-3. Types of Neoplasms Linked to Pulmonary<br />
Metastatic Disease, by Indication for Surgical Metastasectomy<br />
Indicated Controversial Generally Not Indicated<br />
(increases (may increase (likely has no impact<br />
survival) survival) on survival)<br />
Osteogenic Wilm Tumor Neuroblastoma<br />
sarcoma<br />
Alveolar soft Ewing sarcoma Rhabdomyosarcoma<br />
part sarcoma<br />
Adrenocortical Hepatoblastoma Differentiated<br />
carcinoma<br />
thyroid cancer<br />
Figure <strong>96</strong>-10. Computed tomography scan (axial) of a very<br />
small right-sided lung lesion (arrow) typical of metastatic<br />
osteogenic sarcoma.<br />
classically, the lesions associated with osteogenic sarcoma can be<br />
very small (
1648 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
can accommodate the repair, which includes closure of the<br />
sternal defect, repair of the diaphragmatic hernia, and closure of<br />
the omphalocele. 30<br />
Pectus Excavatum<br />
Pectus excavatum accounts for approximately 90% of chest wall<br />
defects, with an incidence of 1 in 300 live births. The etiology is<br />
possibly related to the overgrowth of cartilage in the adjacent ribs,<br />
displacing the sternum posteriorly. Clinically, it presents more<br />
commonly in boys at a ratio of 3:1, becoming more progressive in<br />
posterior displacement as the child enters puberty. It is associated<br />
with Marfan’s syndrome (2% of cases), diaphragmatic abnormalities<br />
(2% of cases) and congenital heart disease (1.5%). 31<br />
Patients may present asymptomatically or may have complaints of<br />
chest pain, palpitations, and asthma-like symptoms. There<br />
continues to be considerable debate about the clinical impact of<br />
this defect upon cardiovascular and pulmonary function.<br />
Intuitively, the compression of the heart and the lungs by the<br />
sternum should result in dysfunction. Lower lung volumes and<br />
decreased cardiac output have been recorded in patients with<br />
severe defects during exercise; 32–33 improvements in function have<br />
been demonstrated in patients postoperatively. Indications for<br />
surgical repair are more commonly psychological, related to issues<br />
around poor self-image, and less commonly related to issues of<br />
physiologic compromise of clinically relevant cardiopulmonary<br />
dysfunction; the latter may be important for a patient with a severe<br />
defect who also happens to be a competitive athlete.<br />
The occasional child with a concurrent diagnosis of Marfan’s<br />
syndrome or congenital heart disease should be considered for<br />
repair of the chest wall defect before open heart surgery to avert<br />
the issues of compression of the cardiac structures. The surgical<br />
options are essentially two: the Ravitch procedure (an open<br />
surgical approach) and the Nuss procedure (a minimally invasive<br />
approach). The former technique has been used for more than 50<br />
years and has undergone minor revisions over time. Figure<br />
<strong>96</strong>–11AB shows a patient with pectus excavatum before and after<br />
a Ravitch repair. Intraoperative and postoperative considerations<br />
include pneumothorax, hemorrhage, and pain management. In<br />
long-term follow-up, patients will experience minor recurrences of<br />
the defect in 10 to 15% of cases and major recurrences in 10 to<br />
15% of cases for an overall recurrence rate of 20 to 30%. 34–35<br />
Because of an infrequent but devastating long-term complication<br />
of thoracic dystrophy, children should be at least 6 years of age<br />
before undergoing surgical correction of this defect; some authors<br />
now recommend delaying repair until 12 to 16 years of age to<br />
reduce the chance of this complication. 36<br />
The Nuss procedure has become the de facto procedure for the<br />
correction of pectus excavatum in the United States. The attraction<br />
of this technique is its cosmetically more acceptable outcome,<br />
because it eliminates the transverse chest incision of the Ravitch<br />
procedure and replaces it with two small lateral chest wall<br />
incisions; it functions on the premise that the chest wall can be<br />
remodeled over a nondeformable metal bar that forcibly pushes<br />
the sternum and ribs from the spine, increasing the anteriorposterior<br />
distance; the bar is usually left in place for 2 to 3 years to<br />
reduce the chance of recurrence of the defect. The intraoperative<br />
and postoperative considerations include pain management,<br />
pneumothorax, and metal bar displacement. More serious<br />
complications have included cardiac perforation, empyema,<br />
pericarditis, and the development of thoracic outlet syndrome.<br />
The overall complication rate is 20 to 28%, which is higher than for<br />
the Ravitch procedure (
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1649<br />
A<br />
Figure <strong>96</strong>-12. A and B: This series demonstrates a patient with pectus carinatum before and after a Ravitch repair (looking from the<br />
side of the patient).<br />
B<br />
defects may result in changes in pulmonary function, which<br />
should be assessed with a complete set of PFTs.<br />
The classical surgical treatment is similar to the approach for<br />
pectus excavatum with a Ravitch repair. This treatment, which<br />
usually yields a very good cosmetic result, is associated with a<br />
transverse scar across the low3er portion of the chest; figure <strong>96</strong>–<br />
12AB shows a patient with pectus carinatum before and after a<br />
Ravitch repair. As such, some authors have advocated the use of<br />
orthotic compression bracing of the chest wall to induce<br />
remodeling of the underlying ribs and sternum. 42–43 One of these<br />
studies found that the bracing led to positive outcomes, provided<br />
that the patients were compliant with wearing their compression<br />
vests. The difficulty with compliance was the requirement to wear<br />
the compression vest for 14 to 16 hours a day for 24 months. 44 The<br />
role of surgical intervention in this chest wall abnormality will<br />
likely decrease over time as the nonoperative options of bracing<br />
becomes more accepted and will only be reserved for children and<br />
adolescents who are noncompliant with the bracing regimen.<br />
DIAPHRAGMATIC ANOMALIES<br />
Among diaphragmatic anomalies, the most common are<br />
Bochdalek (or posteriolateral) congenital diaphragmatic hernias,<br />
at an incidence of 1 in 4000-5000 live births/year. This specific<br />
topic will be reviewed and discussed in <strong>Chapter</strong> 85. Other<br />
anomalies of the diaphragm, including Morgagni diaphragmatic<br />
hernias and diaphragmatic eventrations, will be discussed below.<br />
All of these hernias develop as a result of an abnormality of<br />
embryological development. The diaphragm, whereby the<br />
pleuroperitoneal cavity is separated into two distinct cavities,<br />
usually forms between 4 and 8 weeks of gestation. The diaphragm<br />
is normally composed of a central tendon and a peripheral<br />
muscular section; the former arises from the transverse septum<br />
and the latter arises from the posterolateral pleuroperitoneal folds.<br />
Some diaphragmatic anomalies form as a result of failure of fusion<br />
of the septum and folds; others arise from defects in formation of<br />
the diaphragmatic muscle itself. Morgagni diaphragmatic hernias<br />
develop as a failure of fusion in which the anterior diaphragm<br />
muscle attaches to the sternum.<br />
Morgagni Diaphragmatic Hernia<br />
Morgagni diaphragmatic hernias account for approximately 2%<br />
of all congenital diaphragmatic hernias. They occur in the anterior<br />
midline directly posterior to the sternum or in the parasternal<br />
location through the foramen of Morgagni. Unlike the classical<br />
Bochdalek congenital diaphragmatic hernia, these hernias usually<br />
present with features of intestinal obstruction instead of<br />
respiratory compromise. Usually, children are older when they<br />
become symptomatic, or defects are discovered incidentally on<br />
chest imaging. The hernia sac often contains a portion of the liver<br />
and transverse colon; occasionally it can also contain the small<br />
bowel and stomach, depending on size. These diaphragmatic<br />
defects can be surgically treated with open and laparoscopic<br />
techniques, including either primary closure of the defect or<br />
placement of a synthetic patch. The MAS approach has become<br />
the operation of choice for patients, who are not in any respiratory<br />
distress and can tolerate peritoneal CO 2<br />
insufflation. Surgical<br />
repair involves a laparoscopic approach with either primary<br />
closure of the defect or placement of a synthetic patch. Video<br />
2 demonstrates a laparoscopic view of a moderately-sized<br />
Morgagni hernia. Various authors have successfully applied this<br />
technique 45–46 ; in addition to primary closure of these defects,<br />
some of the authors were able to repair them with prosthetic<br />
patches with only one recurrence in long-term follow-up.<br />
Diaphragmatic Eventration<br />
Diaphragmatic eventration, which usually presents with unilateral<br />
elevation of a hemidiaphragm, can present as congenital or<br />
acquired disease. The former is a result of a defect in adequate<br />
muscularization of the diaphragm; in this case, the diaphragm is<br />
abnormally thin, often lacking muscle and being membranous in<br />
quality. 47 The latter is usually a result of iatrogenic injury of the<br />
phrenic nerve from surgery or from direct invasion of the phrenic<br />
nerve by a neoplasm; in this case, the diaphragmatic muscle is<br />
normal in quality. A portion of or all of the hemidiaphragm may<br />
be involved. The diagnosis can be made on history, especially in<br />
the case of acquired disease. Although most children with
1650 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
congenitally-acquired disease may be asymptomatic, patients with<br />
acquired disease may be symptomatic from a respiratory perspective,<br />
owning to the acute change in diaphragmatic function.<br />
The diagnosis, regardless of etiology, can be assessed with<br />
diagnostic imaging tests, including ultrasound and fluoroscopy of<br />
the diaphragm, looking for paradoxical motion of the diaphragm.<br />
In the event that the diagnosis continues to be unclear, an upper<br />
gastrointestinal series can be obtained. Once a diagnosis is<br />
secured, the option of surgical repair is generally considered for all<br />
patients who are symptomatic and those patients who are<br />
asymptomatic but also have a markedly elevated hemidiaphragm<br />
that is compressing the ipsilateral lung. The surgical procedure<br />
involves plication of involved diaphragm; infrequently, a<br />
redundant portion of the diaphragm will have to be excised. The<br />
approach can be via abdominal or thoracic approach and can be<br />
via an open or thoracoscopic/laparoscopic technique. The latter<br />
technique has been slowly gaining favor among surgeons. A<br />
number of case reports and small case series have been published<br />
that advocate for the use of the laparoscopic/thoracoscopic<br />
techniques. 48 A study by Sato et al. noted that all of the cases were<br />
successfully completed with the thoracoscopic technique and there<br />
were no recurrences in long term follow-up.<br />
ANOMALIES OF THE<br />
LUNG AND AIRWAY<br />
Anomalies of the lung and airway are an area of pediatric surgery<br />
that is undergoing changes with respect to optimal treatment and<br />
management. Some authors have suggested that not all of these<br />
lesions need to be surgically excised and some can be safely<br />
monitored. 49 Aziz et al. have suggested that asymptomatic<br />
congenital cystic adenomatoid malformations can be observed.<br />
Other authors, such as Azizkhan et al., have suggested that all of<br />
these asymptomatic lesions be surgically excised. 50 This remains a<br />
very controversial area and there remains considerable disagreement<br />
on this topic. This section will focus on the current<br />
treatment options for these largely congenital anomalies and will<br />
mention areas of controversy where it alters clinical management;<br />
included in this section is a discussion of spontaneous pneumothorax,<br />
which may be congenital or acquired in origin.<br />
Congenital Pulmonary<br />
Airway Malformation<br />
These lesions are referred to as congenital cystic adenomatoid<br />
malformations (CCAMs) or more recently as congenital<br />
pulmonary airway malformations (CPAMs). They can be<br />
macrocystic, macrocytic, or solid masses which may involve all or<br />
a portion of the lobe of the lung; they communicate with the<br />
airway and usually do not have anomalous blood vessels. There<br />
are a number of histologic subtypes, which embryologically<br />
contain no cartilage and arise from the excessive proliferation of<br />
bronchial structures without alveoli. 51 These lesions are now<br />
diagnosed in three clinical settings: (1) on antenatal ultrasound<br />
examination, (2) when the child presents with symptoms related<br />
to respiratory distress or pulmonary infection (pneumonia and/<br />
or intrapulmonary abscess), or (3) when the lung anomaly is<br />
discovered incidentally on diagnostic chest imaging. The<br />
former examinations have demonstrated that these lesions can<br />
have dramatically distinct clinical courses, including complete<br />
resolution of the lesion before birth, little change in the size of the<br />
lesion, progressive enlargement of the lesion, and in utero demise<br />
related to compression of the heart with impairment of central<br />
venous return, ultimately leading to hydrops.<br />
The primary preoperative indications for surgical resection<br />
of these lesions are: (1) respiratory distress from direct compression<br />
of adjacent intrathoracic structures, (2) prevention of<br />
pulmonary infection (or recurrent pulmonary infection), and (3)<br />
prevention of possible pulmonary malignancy. The latter<br />
indication is one of the most controversial, because it is unclear<br />
whether these malignancies have arisen from a benign congenital<br />
lung lesion or whether the diagnosis of the benign congenital lung<br />
lesion has been in error and the lesion is, in fact, a malignancy.<br />
These lesions are optimally assessed with CT scan imaging,<br />
although ultrasound can be used for lesions that are fluid-filled or<br />
solid and are adjacent to the chest wall. Figure <strong>96</strong>–13 illustrates a<br />
CPAM in the right chest that is primarily cystic with a small solid<br />
component. The surgical approach usually involves complete<br />
resection of the congenital lesion including the surrounding lobe<br />
of the lung via an open or thoracoscopic technique. The latter<br />
technique has been advanced with devices that effectively seal<br />
large vessels and can also go through a 5-mm port; the stapling<br />
devices that are now available are too long for most hemithoraces<br />
in small children and require a 12-mm port. In addition, it<br />
has become common for pediatric surgeons to use low-pressure<br />
intrathoracic insufflation (3–7 mmHg) to safely compress<br />
the ipsilateral lung, instead of one-lung ventilation. which is<br />
prone to technical difficulty given the small airways of children.<br />
Various authors have reported low conversion rates to open<br />
procedures and overall good success rates with the approach.<br />
Albanese et al. have noted maximal conversion rates of 2%, few<br />
other intraoperative complications, and lower mean hospital<br />
lengths of stay. 52<br />
Figure <strong>96</strong>-13. Computed tomography scan (axial) of a congenital<br />
pulmonary airway malformation in the right chest, which is<br />
primarily cystic with a small solid component.
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1651<br />
Pulmonary Sequestration<br />
These lesions are also referred to as bronchopulmonary<br />
sequestrations (BPSs). They classically have anomalous arterial<br />
and pulmonary or systemic venous blood supply and do not<br />
formally communicate with the normal tracheobronchial tree. The<br />
former arterial vessels which arise from the thoracic (85–90%) or<br />
abdominal aorta (10–15%) can be very large, resulting in a large<br />
arteriovenous shunt and possible high-output cardiac failure;<br />
moreover, these vessels, if not properly ligated and divided at the<br />
time of surgical resection, can result in major intraoperative<br />
hemorrhage and can occasionally retract into the subdiaphragmatic<br />
space (if they originate from the abdominal aorta).<br />
There are two types of BPS, intralobar BPS and extralobar BPS.<br />
They differ based on their location within the lung parenchyma;<br />
intralobar BPS, which is more common (making up 90% of BPS),<br />
lies within the parenchyma of the lobe and indirectly communicates<br />
with the adjacent normal lung parenchyma via the<br />
pores of Kohn; these pores create an opportunity for infection of<br />
the BPS. Extralobar BPS is separate from the adjacent lung<br />
parenchyma and is invested with its own visceral pleura but does<br />
similarly have systemic arterial and pulmonary or systemic blood<br />
supplies. As such, it rarely becomes infected but is at risk for<br />
creating an arteriovenous shunt, causing high-output cardiac<br />
failure. Unlike intralobar BPS, extralobar BPS is associated with<br />
congenital diaphragmatic hernias and can be anatomically located<br />
in the thorax (more commonly on the left side) or the subdiaphragmatic<br />
space.<br />
BPS lesions can be imaged with transthoracic ultrasound, chest<br />
CT scan, or MRI. These lesions tend to occur more in the lower<br />
portion of the chest; they are differentiated from other congenital<br />
lesions by identification of a lung mass with an adjacent large<br />
arterial vessel which can be followed to the aorta. Preoperative<br />
indications for surgical resection of intralobar and extralobar BPS<br />
include recurrent pulmonary infection, congestive heart failure,<br />
or resection for diagnosis of a paraspinal mass (to differentiate if<br />
from a neoplasm as a neurogenic tumor). As with CCAM/CPAM,<br />
they can be resected via open or thoracoscopic techniques and<br />
authors have noted equal success with resection of these lesions<br />
with minimal access techniques. 52 Intraoperative considerations<br />
include the rare risk of major hemorrhage if the arterial blood<br />
vessel if not properly ligated; moreover, approximately 15% of BAS<br />
lesions will have more than one arterial blood vessel which can be<br />
inadvertently missed leading to unanticipated blood loss. 51<br />
Congenital Lobar Emphysema<br />
Congenital lobar emphysema (CLE) has multiple etiologies that<br />
lead to overdistention (air trapping) of the lobe of lung, resulting<br />
in compression of adjacent normal lung parenchyma. Some have<br />
implicated the embryologic absence of cartilage in the involved<br />
bronchus, leading to a ball-valve effect of progressive over inflation<br />
of the lung tissue, and others have implicated the polyalveolar lobe<br />
syndrome, which involves the development of abnormally high<br />
numbers of alveoli, leading to gigantic alveolar units. 51 Clinically,<br />
these children present with respiratory symptoms such as<br />
tachypnea; some of these symptoms will resolve with time averting<br />
the need for surgery. Optimal diagnostic imaging is achieved with<br />
a chest CT scan; the upper and middle lobes are most commonly<br />
involved. Figure <strong>96</strong>–14 illustrates a child with left-sided CLE on<br />
CT scan. Bronchoscopy can also be used to identify abnormal areas<br />
Figure <strong>96</strong>-14. Computed tomography scan (axial) of a child<br />
with left-sided, posterior congenital lobar emphysema with<br />
compression of adjacent normal lung parenchyma.<br />
of absent cartilage in the tracheobronchial tree. Intraoperative<br />
complications can occur at the time of induction of anesthesia,<br />
because positive pressure ventilation can cause acute over<br />
distention of the lobe involved with CLE. Strong consideration<br />
should be given to an anesthetic based on spontaneous ventilation<br />
and the surgeon should be in the operating room at the time of<br />
induction in case an emergent thoracotomy is required to relieve<br />
compression of adjacent intrathoracic structures.<br />
Bronchogenic Cysts<br />
Bronchogenic cysts are noncommunicating cystic structures<br />
adjacent to the tracheobronchial tree which usually exist at the<br />
level of the carina or main stem bronchi. They lack normal<br />
alveolar structures but do contain a ciliated columnar epithelial<br />
lining that produces mucus; as the cyst collects mucus, it<br />
extrinsically compressed the adjacent normal bronchial structures.<br />
Although this compression can cause air trapping, resulting in a<br />
clinical picture of CLE, many of these cysts are asymptomatic at<br />
diagnosis and are only noted incidentally on diagnostic chest<br />
imaging. Preoperative indications include surgical excision of the<br />
cysts to address respiratory compromise, to prevent infection of<br />
the cyst, to prevent the unusual occurrence of acute hemorrhage<br />
into the cyst causing acute extrinsic compression of the trachea,<br />
and to prevent the rare case of adenocarcinoma. These patients<br />
are often ideal candidates for a thoracoscopic approach for<br />
resection of the cyst, provided that the ipsilateral lung is not<br />
over inflated. Many authors have demonstrated the benefit of<br />
thoracoscopic resection over open thoracotomy. 53–55 The<br />
complication of injuring the adjacent airway at the time of<br />
resection is now lessened as it is recognized that the entire cyst<br />
wall need not be resected to achieve a low recurrence rate, if the<br />
remaining mucosal lining is cauterized.
1652 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
Spontaneous Pneumothorax<br />
Spontaneous pneumothoraces arise from the rupture of apical<br />
pulmonary blebs in lung parenchyma without underlying disease.<br />
The incidence of this disease is higher in boys with an incidence<br />
of 7 to 18/100,000 in boys and 1 to 6/100,000 in girls. 56 Classically,<br />
the patient is a thin, tall teenage boy who presents with unilateral<br />
chest pain and cough. Although some patients may be more<br />
symptomatic related to significant pulmonary collapse and/or<br />
tension pneumothorax, most are clinically very stable. The<br />
diagnosis is confirmed with a chest radiograph. Although small,<br />
nonincreasing pneumothoraces many resolve with the application<br />
of increase O 2<br />
via nasal prongs or face mask, larger or increasing<br />
pneumothoraces will require placement of a chest tube. As part of<br />
the assessment, a chest CT scan should be obtained to determine<br />
the quality and quantity of apical blebs.<br />
Indications for surgical intervention are: (1) persistent air leak<br />
after 5 to 7 days of chest tube suction, (2) recurrence of the<br />
pneumothorax, and (3) the presence of bilateral or large blebs.<br />
The recurrence rate for spontaneous pneumothorax after the<br />
first spontaneous pneumothorax is highest for teenagers and<br />
approaches 60%. 56 There are three approaches for surgical<br />
treatment: (1) open thoracotomy, (2) transaxillary minithoracotomy,<br />
and (3) thoracoscopy. All involve resection of the<br />
apical lung tissue containing the blebs and pleurodesis of the apex<br />
of the parietal pleura by means of mechanical abrasion, application<br />
of a chemical sclerosant, or apical parietal pleurectomy. The trend<br />
in surgical management has been towards thoracoscopy and away<br />
from transaxillary minithoracotomy. 57,58 One retrospective study<br />
by Butterworth et al. demonstrated a lower postoperative narcotic<br />
requirement, shorter length of hospital stay, and no difference in<br />
recurrence rates for thoracoscopy compared to transaxillary<br />
minithoracotomy. 59 In a large series by Rogers et al., the thoracoscopic<br />
technique had no complications and a low recurrence<br />
rate of 7.4%. 60<br />
EMPYEMA<br />
This disease refers to the accumulation of infected, purulent fluid<br />
in the pleural space. It is often secondary to a bacterial pneumonia,<br />
may occur after thoracic surgery, may be a complication of<br />
trauma, or may be related to other underlying pulmonary diseases.<br />
Empyemas go through three distinct stages; they include (in<br />
order): exudative, fibropurulent, and organizing stages. 61<br />
Management of this disease has undergone multiple iterations;<br />
indications for surgical intervention, as opposed to conservative<br />
management with chest tube drainage, antibiotics, and instillation<br />
of fibrinolytics, have changed over time and have been assessed in<br />
various studies. In the past, the primary surgical approach<br />
involved a classical posteriolateral thoracotomy followed by<br />
removal of the peel of the organized parapneumonic collection;<br />
this procedure was associated with significant intraoperative and<br />
postoperative hemorrhage. When this approach was further<br />
modified to a limited, muscle-sparing thoracotomy, it was better<br />
tolerated by patients. It was advocated that it should be used at an<br />
earlier time in the treatment of the empyema and this approach<br />
was found to decrease the overall morbidity when compared to<br />
conservative management strategies. 62<br />
Subsequently, a thoracoscopic debridement approach was<br />
suggested as a less invasive means of achieving a better clinical<br />
outcome with less morbidity. It has become a first-line therapy for<br />
the management of empyema and is especially efficacious in the<br />
exudative-fibropurulent stages of the disease. 63 The evidence<br />
behind this change includes a study which demonstrated that<br />
children who received thoracoscopic debridement early in the<br />
management of their empyema had no failures, as defined by a<br />
need for open thoracotomy, and had a shorter hospital length of<br />
stay; historical controls who were treated with chest tube drainage<br />
alone had a longer hospital length of stay; some required a delayed<br />
thoracoscopic debridement and a few ultimately required an open<br />
thoracotomy. 64 Other authors have advocated primary use of<br />
thoracoscopic debridement, because it was associated with lower<br />
overall hospital costs, when it was compared to patients who<br />
received conservative chest tube drainage, some of whom would<br />
fail, requiring a delayed thoracoscopic debridement procedure;<br />
the costs of the primary operations were off set by the longer<br />
hospital length of stays in the conservatively managed patients. 65<br />
Despite a relatively large amount of data supporting early<br />
thoracoscopic debridement, the application of this clinical<br />
approach remains very controversial and has not been well<br />
accepted by all clinicians; practices very greatly between and<br />
within institutions.<br />
TRAUMATIC THORACIC INJURIES<br />
Thoracic injuries are the second most common cause of mortality<br />
in children, with a rate of 15 to 22% among hospitalized patients. 66<br />
When combined with other concurrent injuries, the mortality rate<br />
increases to as high as 40%, 43%, and 50% for cardiac, esophageal,<br />
and vascular injuries, respectively (U.S. National Trauma Registry<br />
data, 1985–1991). Blunt traumatic injuries outnumber penetrating<br />
injuries by a factor of greater than 4:1. Approximately 75% of blunt<br />
injuries are a result of motor vehicular collision, with the child as<br />
an occupant of the vehicle or as a pedestrian who is struck by a<br />
vehicle. Specific differences in the anatomy of the child allow for<br />
unique physiologic responses to injuries of the thorax compared<br />
to adults. These differences include a smaller airway that is more<br />
susceptible to obstruction, a larynx that is tilted in a cephalad<br />
direction, making inadvertent esophageal intubation more<br />
common, and a short trachea, making right bronchial intubations<br />
more possible. In addition, the chest wall is more compliant,<br />
allowing for less protection of the intrathoracic organs, and the<br />
mediastinum is more mobile, allowing for a higher chance of a<br />
tension pneumothorax developing with the right clinical<br />
TABLE <strong>96</strong>-4. Injuries to the Thorax, by Likelihood of<br />
Resulting Death<br />
Life-Threatening Potentially Life- Serious<br />
Injuries Threatening Injuries Injuries<br />
Airway injuries Major pulmonary Pneumothorax<br />
contusion<br />
Tension Tracheobronchial Traumatic<br />
pneumothorax injuries asphyxia<br />
Massive hemothorax Myocardial contusion Hemothorax<br />
Cardiac tamponade Diaphragmatic rupture<br />
Flail chest<br />
Esophageal rupture<br />
Open pneumothorax Aortic rupture
CHAPTER <strong>96</strong> ■ Thoracic Surgery: Surgical Considerations 1653<br />
TABLE <strong>96</strong>-5. Various Thoracic Injuries, by Indication<br />
for Surgical Intervention<br />
Emergent or Urgent<br />
Thoracotomy<br />
Massive, persistent pneumothorax<br />
(related to tracheobronchial<br />
injury)<br />
Massive hemothorax<br />
Cardiac tamponade<br />
Open pneumothorax<br />
Esophageal rupture<br />
Vascular injury<br />
Rupture of the diaphragm a<br />
Delayed Thoracotomy<br />
Chronic rupture of the<br />
diaphragm<br />
Chylothorax<br />
Chronic hemothorax<br />
Removal of foreign bodies<br />
a<br />
In the setting of a rupture of the diaphragm, it is important to recognize that the<br />
risk of a concurrent intra-abdominal injury is high enough to warrant repair of<br />
the diaphragm via a laparotomy so that other intra-abdominal injuries can be<br />
simultaneously assessed.<br />
conditions. It should be noted that a child with rib fractures<br />
signifies that a major amount of force has been applied to the<br />
chest, and there needs to be a high index of suspicion of<br />
concurrent injury to the lung, heart, and other mediastinal<br />
structures.<br />
Thoracic injuries can be categorized by the degree to which<br />
they threaten the child’s life (Table <strong>96</strong>–4). Indications for surgical<br />
intervention with these injuries can be divided into those that<br />
require emergent or urgent surgery and those which can be<br />
performed in a more delayed fashion (Table <strong>96</strong>–5).<br />
Clinical findings, as indicated by the setting in which the<br />
thoracic injuries have occurred and the observations in the<br />
trauma room and/or critical care unit, dictate the need for<br />
surgery. Survival with cardiac tamponade is highest in children<br />
who have vital signs before arrival in the emergency department<br />
and have single penetrating wounds (stab wounds and lowvelocity<br />
gunshot wounds) and lowest in children who have absent<br />
vital signs in the prehospital setting and have sustained highvelocity<br />
gun shot wounds or blunt trauma. The latter patients have<br />
an overall survival that approached zero. 66 Other clinical findings<br />
for surgery can be determined by the rate of blood loss as<br />
measured via a chest tube. The current indication for a thora -<br />
cotomy in adults is approximately 1500 mL/24 hours acutely.<br />
Similarly, children whose blood loss approaches 25 to 30% of their<br />
blood volume (20–25 mL/kg/24 h) should undergo urgent<br />
thoracotomy to avoid the high mortality associated with ongoing<br />
massive blood loss and required transfusion. Usually, most<br />
children requiring chest surgery would have it via an open<br />
thoracotomy. The role of thoracoscopic surgery has been<br />
recognized as an important adjunct in the management of these<br />
injuries and it is slowly finding a formal position under specific<br />
clinical conditions. 67 In the setting of a patient with stable vital<br />
signs, some authors have reported success rates as high as<br />
89% with the evacuation of residual empyema and hemothoraces<br />
after thoracic injury. 68 Other authors have found thoracoscopy<br />
to be effective in the diagnosis of diaphragmatic injuries (accurate<br />
to 98%) and the management and control of chest tube<br />
hemorrhage (in 82% of the patients where it was used). The use<br />
of the thoracoscopy averted a need for thoracotomy in 62% of<br />
the cases. 69<br />
REFERENCES<br />
1. DaCosta ML, Redmond HP, Boucher-Hayes DJ. The effect of laparotomy<br />
and laparoscopy on the establishment of spontaneous tumor metastases.<br />
Surgery. 1998;124:516–525.<br />
2. DaCosta ML, Redmond HP, Finnegan N. Laparotomy and laparoscopy<br />
differentially accelerate experimental flank tumor growth. Br J Surg.<br />
1998;85:1439–1442.<br />
3. Wexner SD. Postgraduate course on oncology. Society of American<br />
Gastrointestinal and Endoscopic Surgeons (SAGES) Annual Meeting.<br />
Atlanta, Georgia, March 29–April 1, 2000.<br />
4. Waldhausen JHT, Trapper D, Sawin RS. Minimally invasive surgery and<br />
clinical decision–making for pediatric malignancy. Surgical Endoscopy.<br />
2000;14:250–253.<br />
5. Connolly BL, Chait PG, Duncan DS, et al. CT–guided percutaneous<br />
needle biopsy of small lung nodules in children. Pediatr Radiol.<br />
2000;29:342–346.<br />
6. Hayes–Jordan A, Daw NC, Furman WL, et al. Tumor recurrence at<br />
thoracoscopic tube insertion sites: a report of 2 pediatric cases. J Pediatr<br />
Surg. 2004;39:1565–1567.<br />
7. Rothenberg SS. Thoracoscopic lung resection in children. J Pediatr Surg.<br />
2002;35:271–275.<br />
8. Waters DJ, Coakley FV, Cohen MD, et al. The detection of pulmonary<br />
metastases by helical CT: a clinicopathologic study in dogs. J Comput<br />
Assist Tomogr. 1998;22:235–240.<br />
9. Cirino LM, Milanez de Campos JR, Fernandez A, et al. Diagnosis and<br />
treatment of mediastinal tumors by thoracoscopy. Chest. 2000;117:1787–<br />
1792.<br />
10. Esposito G. Diagnosis of mediastinal masses, principles of surgical tactics<br />
and techniques for their treatment. Semin Pediatr Surg. 1999;8:54–60.<br />
11. Glick RD, LaQuaglia MP. Lymphomas of the anterior mediastinum. Semin<br />
Pediatr Surg. 1999;8:69–77.<br />
12. Shamberger RC. Preanesthetic evaluation of children with anterior<br />
mediastinal masses. Semin Pediatr Surg. 1999;8:61–68.<br />
13. Suzuki K, Nagai K, Yoshida J, Ohmatsu H, et al. Video–assisted<br />
thoracoscopic surgery for small indeterminate pulmonary nodules. Chest.<br />
1999;115:563–568.<br />
14. Holcomb GW III. Minimally invasive surgery for solid tumors. Semin<br />
Surg Oncol. 1999;16:184–192.<br />
15. Hazelrigg SR, Boley TM, Krasna MJ, et al. Thoracoscopic resection of<br />
posterior neurogenic tumors. Am Surg. 1999;65:1129–1133.<br />
16. Sue K, Yamanaka K, Nakamura M. Thoracoscopic resection of ganglioneuroma<br />
in the posterior media. Pediatr Surg Int. 1998;14:151–160.<br />
17. Lacreuse I, Valla JS, de Lagausie P, et al. Thoracoscopic resection of<br />
neurogenic tumors in children. J Pediatr Surg. 2007;42:1725–1728.<br />
18. Grosfeld JL, Skinner MA, Rescoral FJ, et al. Mediastinal tumors in<br />
children: experience with 1<strong>96</strong> cases. Ann Surg Oncol. 1994;1:121–127.<br />
19. Shamberger RC, Holzman RS, Griscom NT, et al. CT quantitation of<br />
tracheal cross–sectional area as a guide to the surgical and anesthetic<br />
management of children with anterior mediastinal masses. J Pediatr Surg.<br />
1991;26:138–142.<br />
20. Hack HA, Wright NB, Wynn RF. The anaesthetic management of children<br />
with anterior mediastinal masses. Anaesthesia. 2008;63:837–846.<br />
21. Slinger P, Karsli C. Management of the patient with a large anterior<br />
mediastinal mass: recurring myths. Curr Opin Anaesthesiol. 2007;20:1–3.<br />
22. Borenstein SH, Gerstle T, Malkin D, et al. The effects of prebiopsy<br />
corticosteroid treatment on the diagnosis of mediastinal lymphoma.<br />
J Pediatr Surg. 2000;35:973–976.<br />
23. Laberge JM. Neuroblastoma. In: Principles of Pediatric Surgery. O'Neill JA<br />
Jr, Grosfeld JL, Fonkalsrud EW, et al, editors. 2nd ed. St Louis: Mosby;<br />
2004. pp. 211–219.<br />
24. Shamberger RC. Teratomas and germ cell tumors. In: Principles of<br />
Pediatric Surgery. O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed. St Louis:<br />
Mosby; 2004. pp. 259–268.<br />
25. Grosfeld J.L. Cervical Cysts, Sinuses, and Other Neck Lesions. In:<br />
Principles of Pediatric Surgery. O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed.<br />
St Louis: Mosby; 2004. pp. 295–297.<br />
26. van den Berg H, van Rijn RR, Merks JH. Management of tumors of the chest<br />
wall in childhood: a review. J Pediatr Hematol Oncol. 2008;30:214–221.<br />
27. Grosfeld JL, Rescorla FJ, West KW, et al. Chest wall resection and<br />
reconstruction for malignant conditions in childhood. J Pediatr Surg.<br />
1988;23:667–673.
1654 PART 5 ■ Anesthetic, Surgical, and Interventional Procedures: Considerations<br />
28. Dishop MK, Kuruvilla S. Primary and metastatic lung tumors in the<br />
pediatric population: a review and 25–year experience at a large children’s<br />
hospital. Arch Pathol Lab Med. 2008;132:1079–1103.<br />
29. Kayton ML. Pulmonary metastasectomy in pediatric patients. Thorac Surg<br />
Clin. 2006;16:167–183.<br />
30. Shamberger RC. Chest wall deformities. In: Principles of Pediatric Surgery.<br />
O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed. St Louis: Mosby; 2004. pp.<br />
367–369.<br />
31. Shamberger RC, Welch KJ. Surgical repair of pectus excavatum. J Pediatr<br />
Surg. 1988;23:615–622.<br />
32. Bevegard S. Postural circulatory changes at rest and during exercise in<br />
patients with funnel chest, with special reference to factors affecting the<br />
stroke volume. Acta Med Scand. 1<strong>96</strong>2;171:695.<br />
33. Orzalesi MM, Cook CD. Pulmonary function in children with pectus<br />
excavatum. J Pediatr. 1<strong>96</strong>5;66:898.<br />
34. Hecher WC, Rocher G, Dietz HG. Results of operative correction of<br />
pigeon and funnel chest following a modified procedure of Ravitch and<br />
Haller. Z Kinderchir. 1981;34:220–227.<br />
35. Willital GH. Operationsindikartion–Operationstechnik bei brustorbdeformierungen.<br />
Z Kinderchir. 1981;33:244–252.<br />
36. Boulanger SC, Glick PL. A miniature access approach to pectus<br />
excavatum. In: Pediatric Minimal Access Surgery. Langer JC, Albanese CT,<br />
editors. Boca Raton: Taylor & Francis; 2005. pp. 337.<br />
37. Miller KA, Woods RK, Sharp RJ, et al. Minimally invasive repair of pectus<br />
excavatum: a single institution’s experience. Surgery. 2001;130:652–659.<br />
38. Molik KA, Engum SA, Rescorla FJ, et al. Pectus excavatum repair:<br />
experience with standard and minimal invasive techniques. J Pediatr Surg.<br />
2001;36:324–328.<br />
39. Nuss D, Kelly RE Jr, Croitoru DP, et al. A 10–year review of a minimally<br />
invasive technique for the correction of pectus excavatum. J Pediatr Surg.<br />
1998;33:545–552.<br />
40. Wu PC, Knauer EM. McGowan, GE, et al. Repair of pectus excavatum<br />
deformities in children: a new perspective of treatment using minimal<br />
access surgical technique. Arch Surg. 2001;136:419–424.<br />
41. Kelly RE Jr, Shamberger RC, Mellins RB, et al. Prospective multicenter<br />
study of surgical correction of pectus excavatum: design, perioperative<br />
complications, pain, and baseline pulmonary function facilitated by<br />
internet–based data collection. J Am Coll Surg. 2007;205:205–216.<br />
42. Banever GT, Konefal SH, Gettens K, et al. Nonoperative correction of<br />
pectus carinatum with orthotic bracing. J Laparoendosc Adv Surg Tech A.<br />
2006;16:164–167.<br />
43. Mavanur A, Hight DW. Pectus excavatum and carinatum: new concepts<br />
in the correction of congenital chest wall deformities in the pediatric age<br />
group. Conn Med. 2008;72:5–11.<br />
44. Frey AS, Garcia VF, Brown RL, et al. Nonoperative management of pectus<br />
carinatum. J Pediatr Surg. 2006;41:40–45.<br />
45. Becmur F, Philippe P, van der Zee D, et al. Laparoscopic surgery of<br />
Morgagni–Larrey hernias: a multicenter study of the groupe d’etude in<br />
coeliochirurgie infantile (GECI). Pediatr Endosurg Innov Tech. 2003;7:<br />
147–152.<br />
46. Hendrickson R, Rothenberg SS, Patrick DB. Laparoscopic repair of<br />
congenital diaphragmatic hernia. J Pediatr Surg. 2002;6:80–91.<br />
47. Stolar CJ. Congenital diaphragmatic hernia. In: Principles of Pediatric<br />
Surgery. O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed. St Louis: Mosby;<br />
2004. pp. 457–463.<br />
48. Sato M, Hamada Y, Takada K, et al. Thoracoscopic diaphragmatic<br />
procedures under artificial pneumothorax. Pediatr Surg Int. 2005;21:<br />
34–38.<br />
49. Aziz D, Langer JC, Tuuha SE, et al. Perinatally diagnosed asymptomatic<br />
congenital cystic adenomatoid malformation: to resect or not? J Pediatr<br />
Surg. 2004;39:329–334.<br />
50. Azizkhan RG, Crombleholme TM. Congenital cystic lung disease:<br />
contemporary antenatal and postnatal management. Pediatr Surg Int.<br />
2008;24:643–657.<br />
51. Shamberger RC. Congenital anomalies of the lung. In: Principles of<br />
Pediatric Surgery. O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed. St Louis:<br />
Mosby; 2004. pp. 339–347.<br />
52. Albanese CT, Sydorak RM, Tsao K, Lee H. Thoracoscopic lobectomy for<br />
prenatally diagnosed lung lesions. J Pediatr Surg. 2003;38:553–555.<br />
53. Gossot D, Izquierdo RR, Girard P, et al. Thoracoscopic resection of<br />
bulky intrathoracic benign lesions. Eur J Cardiothorac Surg. 2007;32:<br />
848–851.<br />
54. Koontz CS, Oliva V, Gow KW, et al. Video–assisted thoracoscopic<br />
surgical excision of cystic lung disease in children. Pediatr Surg. 2005;40:<br />
835–837.<br />
55. Tölg C, Abelin K, Laudenbach V, et al. Open vs thorascopic surgical<br />
management of bronchogenic cysts. Surg Endosc. 2005;19:77–80.<br />
56. Baumann MH, Strange C. Treatment of spontaneous pneumothorax:<br />
a more aggressive approach? Chest. 1997;112:789–804.<br />
57. Langenburg SE, Lelli JL. Minimally invasive surgery of the lung: lung<br />
biopsy, treatment of spontaneous pneumothorax, and pulmonary<br />
resection. Semin Pediatr Surg. 2008;17:30–33.<br />
58. Tsao K, St Peter SD, Sharp SW, et al. Current application of thoracoscopy<br />
in children. J Laparoendosc Adv Surg Tech A. 2008;18:131–135.<br />
59. Butterworth SA, Blair GK, LeBlanc JG, et al. An open and shut case for<br />
early VATS treatment of primary spontaneous pneumothorax in children.<br />
Can J Surg. 2007;50:171–174.<br />
60. Rodgers BM. Pediatric thoracoscopy. Where have we come? What have<br />
we learned? Ann Thorac Surg. 1993;56:704–707.<br />
61. Andrews NC, Parker EF, Shaw RR, et al. Management of nontuberculous<br />
empyema. Am Rev Respir Dis. 1<strong>96</strong>2;85:935–936.<br />
62. Shankar KR, Kenny SE, Okoye BO, et al. Evolving experience in the<br />
management of empyema thoracis. Acta Pediatr. 2000;89:417–420.<br />
63. Cameron B. Minimal access surgery in the management of empyema. In:<br />
Pediatric Minimal Access Surgery. Langer JC, Albanese CT, editors. Boca<br />
Raton: Taylor & Francis; 2005. pp. 310–20.<br />
64. Doski JJ, Lou D, Hicks BA, et al. Management of parapneumonic<br />
collections in infants and children. J Pediatr Surg. 2000;35:265–270.<br />
65. Finck C, Wagner C, Jackson R, et al. Empyema–development of a critical<br />
pathway. Semin Pediatr Surg. 2002;11:25–28.<br />
66. Nakayama DK. Thoracic injuries. In: Principles of Pediatric Surgery.<br />
O’Neill J Jr, Grosfeld J, et al, editors. 2nd ed. St Louis: Mosby; 2004. pp.<br />
150–158.<br />
67. Goldstein AM, Stylianos S. The role of minimal access surgery in pediatric<br />
trauma. In: Pediatric Minimal Access Surgery. Langer JC, Albanese CT,<br />
editors. Boca Raton: Taylor & Francis; 2005. pp. 81–88.<br />
68. Sosa JL, Pombo H, Puento I, et al. Thoracoscopy in the evaluation and<br />
management of thoracic trauma. Int Surg. 1998;83:187–189.<br />
69. Villavincencio RT, Aucar JA, Wall MJ, et al. Analysis of thoracoscopy in<br />
trauma. Surg Endosc. 1999;13:3–9.














