

EUROHEALTH
Eurohealth-volume22-number2-2016
Eurohealth-volume22-number2-2016

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
20<br />
Moving towards universal health coverage<br />
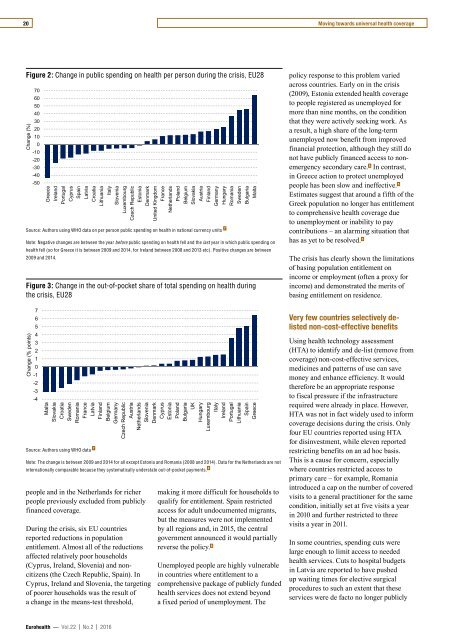
Figure 2: Change in public spending on health per person during the crisis, EU28<br />
Change (%)<br />
70<br />
60<br />
50<br />
40<br />
30<br />
20<br />
10<br />
0<br />
-10<br />
-20<br />
-30<br />
-40<br />
-50<br />
Greece<br />
Ireland<br />
Portugal<br />
Cyprus<br />
Spain<br />
Latvia<br />
Croatia<br />
Lithuania<br />
Italy<br />
Slovenia<br />
Luxembourg<br />
Source: Authors using WHO data on per person public spending on health in national currency units 7<br />
Czech Republic<br />
Estonia<br />
Note: Negative changes are between the year before public spending on health fell and the last year in which public spending on<br />
health fell (so for Greece it is between 2009 and 2014, for Ireland between 2008 and 2013 etc). Positive changes are between<br />
2009 and 2014.<br />
Figure 3: Change in the out-of-pocket share of total spending on health during<br />
the crisis, EU28<br />
Change (% points)<br />
7<br />
6<br />
5<br />
4<br />
3<br />
2<br />
1<br />
0<br />
-1<br />
-2<br />
-3<br />
-4<br />
Malta<br />
Slovakia<br />
Croatia<br />
Sweden<br />
Romania<br />
France<br />
Latvia<br />
Source: Authors using WHO data 7<br />
Finland<br />
Belgium<br />
Germany<br />
Czech Republic<br />
Austria<br />
Netherlands<br />
people and in the Netherlands for richer<br />
people previously excluded from publicly<br />
financed coverage.<br />
Denmark<br />
Slovenia<br />
During the crisis, six EU countries<br />
reported reductions in population<br />
entitlement. Almost all of the reductions<br />
affected relatively poor households<br />
(Cyprus, Ireland, Slovenia) and noncitizens<br />
(the Czech Republic, Spain). In<br />
Cyprus, Ireland and Slovenia, the targeting<br />
of poorer households was the result of<br />
a change in the means-test threshold,<br />
United Kingdom<br />
Denmark<br />
Note: The change is between 2009 and 2014 for all except Estonia and Romania (2008 and 2014). Data for the Netherlands are not<br />
internationally comparable because they systematically understate out-of-pocket payments. 8<br />
France<br />
Cyprus<br />
Netherlands<br />
Estonia<br />
Poland<br />
Poland<br />
Belgium<br />
Bulgaria<br />
Slovakia<br />
UK<br />
Austria<br />
Hungary<br />
Finland<br />
Luxembourg<br />
Germany<br />
Italy<br />
Hungary<br />
Ireland<br />
Romania<br />
Portugal<br />
Sweden<br />
Lithuania<br />
Bulgaria<br />
Spain<br />
Malta<br />
Greece<br />
making it more difficult for households to<br />
qualify for entitlement. Spain restricted<br />
access for adult undocumented migrants,<br />
but the measures were not implemented<br />
by all regions and, in 2015, the central<br />
government announced it would partially<br />
reverse the policy. 6<br />
Unemployed people are highly vulnerable<br />
in countries where entitlement to a<br />
comprehensive package of publicly funded<br />
health services does not extend beyond<br />
a fixed period of unemployment. The<br />
policy response to this problem varied<br />
across countries. Early on in the crisis<br />
(2009), Estonia extended health coverage<br />
to people registered as unemployed for<br />
more than nine months, on the condition<br />
that they were actively seeking work. As<br />
a result, a high share of the long-term<br />
unemployed now benefit from improved<br />
financial protection, although they still do<br />
not have publicly financed access to nonemergency<br />
secondary care. 5 In contrast,<br />
in Greece action to protect unemployed<br />
people has been slow and ineffective. 5<br />
Estimates suggest that around a fifth of the<br />
Greek population no longer has entitlement<br />
to comprehensive health coverage due<br />
to unemployment or inability to pay<br />
contributions – an alarming situation that<br />
has as yet to be resolved. 5<br />
The crisis has clearly shown the limitations<br />
of basing population entitlement on<br />
income or employment (often a proxy for<br />
income) and demonstrated the merits of<br />
basing entitlement on residence.<br />
Very few countries selectively delisted<br />
non-cost-effective benefits<br />
Using health technology assessment<br />
(HTA) to identify and de-list (remove from<br />
coverage) non-cost-effective services,<br />
medicines and patterns of use can save<br />
money and enhance efficiency. It would<br />
therefore be an appropriate response<br />
to fiscal pressure if the infrastructure<br />
required were already in place. However,<br />
HTA was not in fact widely used to inform<br />
coverage decisions during the crisis. Only<br />
four EU countries reported using HTA<br />
for disinvestment, while eleven reported<br />
restricting benefits on an ad hoc basis.<br />
This is a cause for concern, especially<br />
where countries restricted access to<br />
primary care – for example, Romania<br />
introduced a cap on the number of covered<br />
visits to a general practitioner for the same<br />
condition, initially set at five visits a year<br />
in 2010 and further restricted to three<br />
visits a year in 2011.<br />
In some countries, spending cuts were<br />
large enough to limit access to needed<br />
health services. Cuts to hospital budgets<br />
in Latvia are reported to have pushed<br />
up waiting times for elective surgical<br />
procedures to such an extent that these<br />
services were de facto no longer publicly<br />
Eurohealth — Vol.22 | No.2 | 2016













