Dental Asia March/April 2022
For more than two decades, Dental Asia is the premium journal in linking dental innovators and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.
For more than two decades, Dental Asia is the premium journal in linking dental innovators and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CLINICAL FEATURE<br />
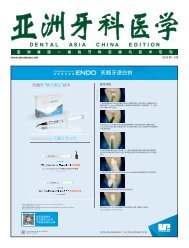
Fig 3b<br />
Fig 3a<br />
Fig 3c<br />
Fig 3d<br />
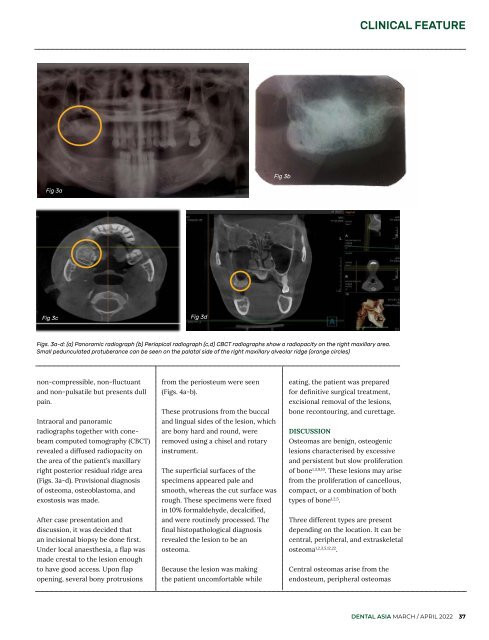
Figs. 3a-d: (a) Panoramic radiograph (b) Periapical radiograph (c,d) CBCT radiographs show a radiopacity on the right maxillary area.<br />
Small pedunculated protuberance can be seen on the palatal side of the right maxillary alveolar ridge (orange circles)<br />
non-compressible, non-fluctuant<br />
and non-pulsatile but presents dull<br />
pain.<br />
Intraoral and panoramic<br />
radiographs together with conebeam<br />
computed tomography (CBCT)<br />
revealed a diffused radiopacity on<br />
the area of the patient’s maxillary<br />
right posterior residual ridge area<br />
(Figs. 3a-d). Provisional diagnosis<br />
of osteoma, osteoblastoma, and<br />
exostosis was made.<br />
After case presentation and<br />
discussion, it was decided that<br />
an incisional biopsy be done first.<br />
Under local anaesthesia, a flap was<br />
made crestal to the lesion enough<br />
to have good access. Upon flap<br />
opening, several bony protrusions<br />
from the periosteum were seen<br />
(Figs. 4a-b).<br />
These protrusions from the buccal<br />
and lingual sides of the lesion, which<br />
are bony hard and round, were<br />
removed using a chisel and rotary<br />
instrument.<br />
The superficial surfaces of the<br />
specimens appeared pale and<br />
smooth, whereas the cut surface was<br />
rough. These specimens were fixed<br />
in 10% formaldehyde, decalcified,<br />
and were routinely processed. The<br />
final histopathological diagnosis<br />
revealed the lesion to be an<br />
osteoma.<br />
Because the lesion was making<br />
the patient uncomfortable while<br />
eating, the patient was prepared<br />
for definitive surgical treatment,<br />
excisional removal of the lesions,<br />
bone recontouring, and curettage.<br />
DISCUSSION<br />
Osteomas are benign, osteogenic<br />
lesions characterised by excessive<br />
and persistent but slow proliferation<br />
of bone 1,3,9,10 . These lesions may arise<br />
from the proliferation of cancellous,<br />
compact, or a combination of both<br />
types of bone 1,2,5 .<br />
Three different types are present<br />
depending on the location. It can be<br />
central, peripheral, and extraskeletal<br />
osteoma 1,2,3,5,12,22 .<br />
Central osteomas arise from the<br />
endosteum, peripheral osteomas<br />
DENTAL ASIA MARCH / APRIL <strong>2022</strong> 37