Diagnosticul imagistic al tumorilor de unghi ponto-cerebelos
Diagnosticul imagistic al tumorilor de unghi ponto-cerebelos
Diagnosticul imagistic al tumorilor de unghi ponto-cerebelos

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
12<br />
Rezumat <strong>Diagnosticul</strong> <strong>imagistic</strong> <strong>al</strong> <strong>tumorilor</strong> <strong>de</strong> <strong>unghi</strong> <strong>ponto</strong>-<strong>cerebelos</strong><br />
*Secţiunile fine hight-resolution sunt utile pentru evi<strong>de</strong>nţierea<br />
modificărilor osoase, dar sunt limitate în abilitatea <strong>de</strong>scoperirii<br />
<strong>tumorilor</strong> mici în conductul auditiv intern<br />
*Tumorile în tot<strong>al</strong>itate extracan<strong>al</strong>are nu dau modificări la nivelul<br />
conductului auditiv intern<br />
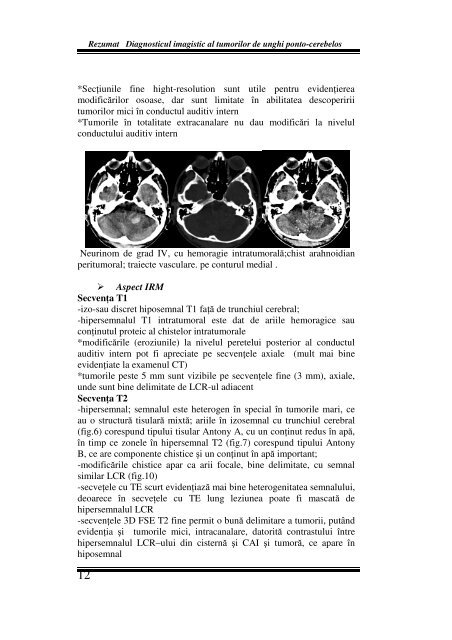
Neurinom <strong>de</strong> grad IV, cu hemoragie intratumor<strong>al</strong>ă;chist arahnoidian<br />
peritumor<strong>al</strong>; traiecte vasculare. pe conturul medi<strong>al</strong> .<br />
Aspect IRM<br />
Secvenţa T1<br />
-izo-sau discret hiposemn<strong>al</strong> T1 faţă <strong>de</strong> trunchiul cerebr<strong>al</strong>;<br />
-hipersemn<strong>al</strong>ul T1 intratumor<strong>al</strong> este dat <strong>de</strong> ariile hemoragice sau<br />
conţinutul proteic <strong>al</strong> chistelor intratumor<strong>al</strong>e<br />
*modificările (eroziunile) la nivelul peretelui posterior <strong>al</strong> conductul<br />
auditiv intern pot fi apreciate pe secvenţele axi<strong>al</strong>e (mult mai bine<br />
evi<strong>de</strong>nţiate la examenul CT)<br />
*tumorile peste 5 mm sunt vizibile pe secvenţele fine (3 mm), axi<strong>al</strong>e,<br />
un<strong>de</strong> sunt bine <strong>de</strong>limitate <strong>de</strong> LCR-ul adiacent<br />
Secvenţa T2<br />
-hipersemn<strong>al</strong>; semn<strong>al</strong>ul este heterogen în speci<strong>al</strong> în tumorile mari, ce<br />
au o structură tisulară mixtă; ariile în izosemn<strong>al</strong> cu trunchiul cerebr<strong>al</strong><br />
(fig.6) corespund tipului tisular Antony A, cu un conţinut redus în apă,<br />
în timp ce zonele în hipersemn<strong>al</strong> T2 (fig.7) corespund tipului Antony<br />
B, ce are componente chistice şi un conţinut în apă important;<br />
-modificările chistice apar ca arii foc<strong>al</strong>e, bine <strong>de</strong>limitate, cu semn<strong>al</strong><br />
similar LCR (fig.10)<br />
-secveţele cu TE scurt evi<strong>de</strong>nţiază mai bine heterogenitatea semn<strong>al</strong>ului,<br />
<strong>de</strong>oarece în secveţele cu TE lung leziunea poate fi mascată <strong>de</strong><br />
hipersemn<strong>al</strong>ul LCR<br />
-secvenţele 3D FSE T2 fine permit o bună <strong>de</strong>limitare a tumorii, putând<br />
evi<strong>de</strong>nţia şi tumorile mici, intracan<strong>al</strong>are, datorită contrastului între<br />
hipersemn<strong>al</strong>ul LCR–ului din cisternă şi CAI şi tumoră, ce apare în<br />
hiposemn<strong>al</strong>