Pragmatische Lösung eines komplexen Problems Schweizer ...
Pragmatische Lösung eines komplexen Problems Schweizer ...
Pragmatische Lösung eines komplexen Problems Schweizer ...

Erfolgreiche ePaper selbst erstellen
Machen Sie aus Ihren PDF Publikationen ein blätterbares Flipbook mit unserer einzigartigen Google optimierten e-Paper Software.
ANZEIGE<br />
The GOG-0218 data also show that<br />
maintenance therapy is important. The<br />
time between the end of chemotherapy<br />
and relapse is crucial and giving bevacizumab<br />
before relapse potentially<br />
provides the opportunity to change the<br />
natural history of disease. Overall, the<br />
data give a positive message; now we<br />
should try to optimise the treatment.<br />
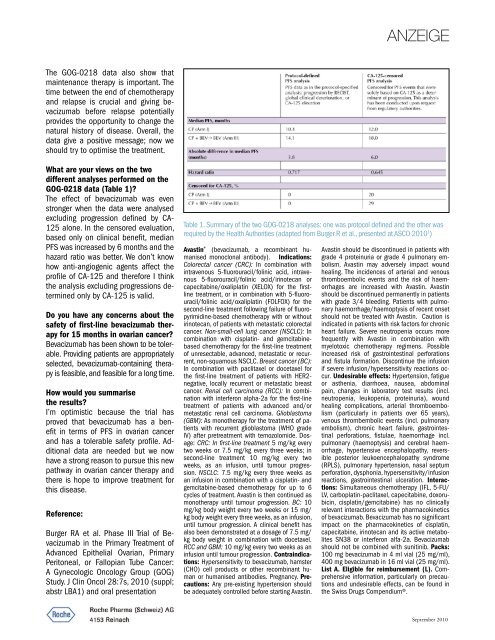
What are your views on the two<br />
different analyses performed on the<br />
GOG-0218 data (Table 1)?<br />
The effect of bevacizumab was even<br />
stronger when the data were analysed<br />
excluding progression defined by CA-<br />
125 alone. In the censored evaluation,<br />
based only on clinical benefit, median<br />
PFS was increased by 6 months and the<br />
hazard ratio was better. We don’t know<br />
how anti-angiogenic agents affect the<br />
profile of CA-125 and therefore I think<br />
the analysis excluding progressions determined<br />
only by CA-125 is valid.<br />
Do you have any concerns about the<br />
safety of first-line bevacizumab therapy<br />
for 15 months in ovarian cancer?<br />
Bevacizumab has been shown to be tolerable.<br />
Providing patients are appropriately<br />
selected, bevacizumab-containing therapy<br />
is feasible, and feasible for a long time.<br />
How would you summarise<br />
the results?<br />
I’m optimistic because the trial has<br />
proved that bevacizumab has a benefit<br />
in terms of PFS in ovarian cancer<br />
and has a tolerable safety profile. Additional<br />
data are needed but we now<br />
have a strong reason to pursue this new<br />
pathway in ovarian cancer therapy and<br />
there is hope to improve treatment for<br />
this disease.<br />
Reference:<br />
Burger RA et al. Phase III Trial of Bevacizumab<br />
in the Primary Treatment of<br />
Advanced Epithelial Ovarian, Primary<br />
Peritoneal, or Fallopian Tube Cancer:<br />
A Gynecologic Oncology Group (GOG)<br />
Study. J Clin Oncol 28:7s, 2010 (suppl;<br />
abstr LBA1) and oral presentation<br />
Table 1. Summary of the two GOG-0218 analyses: one was protocol defined and the other was<br />
required by the Health Authorities (adapted from Burger R et al., presented at ASCO 2010 1 )<br />
Avastin ® (bevacizumab, a recombinant humanised<br />
monoclonal antibody). Indications:<br />
Colorectal cancer (CRC): In combination with<br />
intravenous 5-fluorouracil/folinic acid, intravenous<br />
5-fluorouracil/folinic acid/irinotecan or<br />
capecitabine/oxaliplatin (XELOX) for the firstline<br />
treatment, or in combination with 5-fluorouracil/folinic<br />
acid/oxaliplatin (FOLFOX) for the<br />
second-line treatment following failure of fluoropyrimidine-based<br />
chemotherapy with or without<br />
irinotecan, of patients with metastatic colorectal<br />
cancer. Non-small-cell lung cancer (NSCLC): In<br />
combination with cisplatin- and gemcitabinebased<br />
chemotherapy for the first-line treatment<br />
of unresectable, advanced, metastatic or recurrent,<br />
non-squamous NSCLC. Breast cancer (BC):<br />
In combination with paclitaxel or docetaxel for<br />
the first-line treatment of patients with HER2-<br />
negative, locally recurrent or metastatic breast<br />
cancer. Renal cell carcinoma (RCC): In combination<br />
with interferon alpha-2a for the first-line<br />
treatment of patients with advanced and/or<br />
metastatic renal cell carcinoma. Glioblastoma<br />
(GBM): As monotherapy for the treatment of patients<br />
with recurrent glioblastoma (WHO grade<br />
IV) after pretreatment with temozolomide. Dosage:<br />
CRC: In first-line treatment 5 mg/kg every<br />
two weeks or 7.5 mg/kg every three weeks; in<br />
second-line treatment 10 mg/kg every two<br />
weeks, as an infusion, until tumour progression.<br />
NSCLC: 7.5 mg/kg every three weeks as<br />
an infusion in combination with a cisplatin- and<br />
gemcitabine-based chemotherapy for up to 6<br />
cycles of treatment. Avastin is then continued as<br />
monotherapy until tumour progression. BC: 10<br />
mg/kg body weight every two weeks or 15 mg/<br />
kg body weight every three weeks, as an infusion,<br />
until tumour progression. A clinical benefit has<br />
also been demonstrated at a dosage of 7.5 mg/<br />
kg body weight in combination with docetaxel.<br />
RCC and GBM: 10 mg/kg every two weeks as an<br />
infusion until tumour progression. Contraindications:<br />
Hypersensitivity to bevacizumab, hamster<br />
(CHO) cell products or other recombinant human<br />
or humanised antibodies. Pregnancy. Precautions:<br />
Any pre-existing hypertension should<br />
be adequately controlled before starting Avastin.<br />
Avastin should be discontinued in patients with<br />
grade 4 proteinuria or grade 4 pulmonary embolism.<br />
Avastin may adversely impact wound<br />
healing. The incidences of arterial and venous<br />
thromboembolic events and the risk of haemorrhages<br />
are increased with Avastin. Avastin<br />
should be discontinued permanently in patients<br />
with grade 3/4 bleeding. Patients with pulmonary<br />
haemorrhage/haemoptysis of recent onset<br />
should not be treated with Avastin. Caution is<br />
indicated in patients with risk factors for chronic<br />
heart failure. Severe neutropenia occurs more<br />
frequently with Avastin in combination with<br />
myelotoxic chemotherapy regimens. Possible<br />
increased risk of gastrointestinal perforations<br />
and fistula formation. Discontinue the infusion<br />
if severe infusion/hypersensitivity reactions occur.<br />
Undesirable effects: Hypertension, fatigue<br />
or asthenia, diarrhoea, nausea, abdominal<br />
pain, changes in laboratory test results (incl.<br />
neutropenia, leukopenia, proteinuria), wound<br />
healing complications, arterial thromboembolism<br />
(particularly in patients over 65 years),<br />
venous thrombembolic events (incl. pulmonary<br />
embolism), chronic heart failure, gastrointestinal<br />
perforations, fistulae, haemorrhage incl.<br />
pulmonary (haemoptysis) and cerebral haemorrhage,<br />
hypertensive encephalopathy, reversible<br />
posterior leukoencephalopathy syndrome<br />
(RPLS), pulmonary hypertension, nasal septum<br />
perforation, dysphonia, hypersensitivity/infusion<br />
reactions, gastrointestinal ulceration. Interactions:<br />
Simultaneous chemotherapy (IFL, 5-FU/<br />
LV, carboplatin-paclitaxel, capecitabine, doxorubicin,<br />
cisplatin/gemcitabine) has no clinically<br />
relevant interactions with the pharmacokinetics<br />
of bevacizumab. Bevacizumab has no significant<br />
impact on the pharmacokinetics of cisplatin,<br />
capecitabine, irinotecan and its active metabolites<br />
SN38 or interferon alfa-2a. Bevacizumab<br />
should not be combined with sunitinib. Packs:<br />
100 mg bevacizumab in 4 ml vial (25 mg/ml),<br />
400 mg bevacizumab in 16 ml vial (25 mg/ml).<br />
List A. Eligible for reimbursement (L). Comprehensive<br />
information, particularly on precautions<br />
and undesirable effects, can be found in<br />
the Swiss Drugs Compendium®.<br />
September 2010