

Contents Chapter Topic Page Neonatology Respiratory Cardiology
Contents Chapter Topic Page Neonatology Respiratory Cardiology
Contents Chapter Topic Page Neonatology Respiratory Cardiology

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
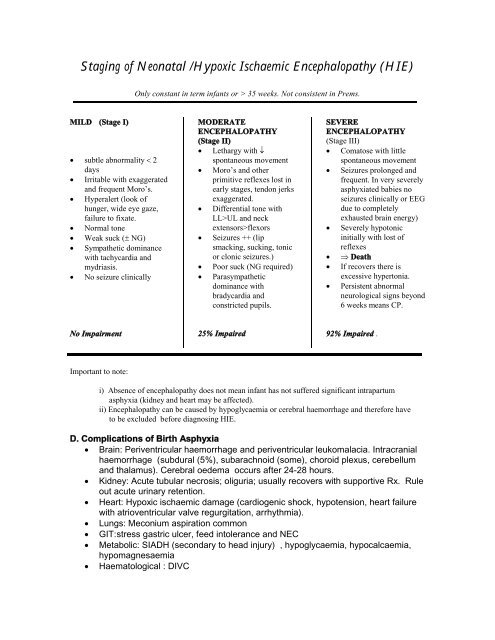
Staging of Neonatal /Hypoxic Ischaemic Encephalopathy (HIE)<br />
MILD (Stage I)<br />
subtle abnormality <br />
days<br />
Irritable with exaggerated<br />
and frequent Moro’s.<br />
Hyperalert (look of<br />
hunger, wide eye gaze,<br />
failure to fixate.<br />
Normal tone<br />
Weak suck ( NG)<br />
Sympathetic dominance<br />
with tachycardia and<br />
mydriasis.<br />
No seizure clinically<br />
No Impairment<br />
Important to note:<br />
Only constant in term infants or > 35 weeks. Not consistent in Prems.<br />
MODERATE<br />
ENCEPHALOPATHY<br />
(Stage II)<br />
Lethargy with <br />
spontaneous movement<br />
Moro’s and other<br />
primitive reflexes lost in<br />
early stages, tendon jerks<br />
exaggerated.<br />
Differential tone with<br />
LL>UL and neck<br />
extensors>flexors<br />
Seizures ++ (lip<br />
smacking, sucking, tonic<br />
or clonic seizures.)<br />
Poor suck (NG required)<br />
Parasympathetic<br />
dominance with<br />
bradycardia and<br />
constricted pupils.<br />
25% Impaired<br />
SEVERE<br />
ENCEPHALOPATHY<br />
(Stage III)<br />
Comatose with little<br />
spontaneous movement<br />
Seizures prolonged and<br />
frequent. In very severely<br />
asphyxiated babies no<br />
seizures clinically or EEG<br />
due to completely<br />
exhausted brain energy)<br />
Severely hypotonic<br />
initially with lost of<br />
reflexes<br />
Death<br />
If recovers there is<br />
excessive hypertonia.<br />
Persistent abnormal<br />
neurological signs beyond<br />
6 weeks means CP.<br />
92% Impaired .<br />
i) Absence of encephalopathy does not mean infant has not suffered significant intrapartum<br />
asphyxia (kidney and heart may be affected).<br />
ii) Encephalopathy can be caused by hypoglycaemia or cerebral haemorrhage and therefore have<br />
to be excluded before diagnosing HIE.<br />
D. Complications of Birth Asphyxia<br />
Brain: Periventricular haemorrhage and periventricular leukomalacia. Intracranial<br />
haemorrhage (subdural (5%), subarachnoid (some), choroid plexus, cerebellum<br />
and thalamus). Cerebral oedema occurs after 24-28 hours.<br />
Kidney: Acute tubular necrosis; oliguria; usually recovers with supportive Rx. Rule<br />
out acute urinary retention.<br />
Heart: Hypoxic ischaemic damage (cardiogenic shock, hypotension, heart failure<br />
with atrioventricular valve regurgitation, arrhythmia).<br />
Lungs: Meconium aspiration common<br />
GIT:stress gastric ulcer, feed intolerance and NEC<br />
Metabolic: SIADH (secondary to head injury) , hypoglycaemia, hypocalcaemia,<br />
hypomagnesaemia<br />
Haematological : DIVC













