

Contents Chapter Topic Page Neonatology Respiratory Cardiology
Contents Chapter Topic Page Neonatology Respiratory Cardiology
Contents Chapter Topic Page Neonatology Respiratory Cardiology

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Hypocalcaemia has 2 major peaks of incidences.<br />
1st peak in first 2 to 3 days of life, usually in low birth weight infants, IDM and infants with HIE of<br />
perinatal asphyxia. A therapeutic response to intravenous calcium is helpful in determining low<br />
serum calcium as a cause of the seizures. It is much more common for early hypocalcaemia to be<br />
an association of early seizures rather than a cause.<br />
Later -onset of hypocalcaemia are associated with endocrinopathy ( maternal hypoparathyroidism,<br />
neonatal hypoparathyroidism) and heart disease ( with or without Di George Syndrome), rarely with<br />
nutritional type ( cow’s milk, high phosphorus synthetic milk). Hypomagnesemia is a frequent<br />
accompaniment.<br />
Other metabolic disturbances include neonatal intoxication with lidocaine, hyponatraemia,<br />
hypernatraemia, amino acidopathy ( nonketotic hyperglycinemia), organic acidopathy,<br />
hyperammonemia, mitochondrial disturbance, perioxisomal disorders, pyridoxine dependency<br />
(recalcitrant seizures ceased with intravenous pyridoxine ) and disorder of glucose transport ( low<br />
glucose in CSF but normal blood glucose, treatment with ketogenic diet)<br />
Seizures versus Jitteriness and Other Non-epileptic Movements<br />
Some movements e.g. jitteriness and other normal movement during sleep<br />
(Myoclonic jerks or generalized myoclonic jerks as infant wakes from sleep) or when<br />
awake/ drowsy (roving sometimes dysconjugate eye movements, sucking not<br />
accompanied by ocular fixation or deviation) in newborn may be mistaken for seizures.<br />
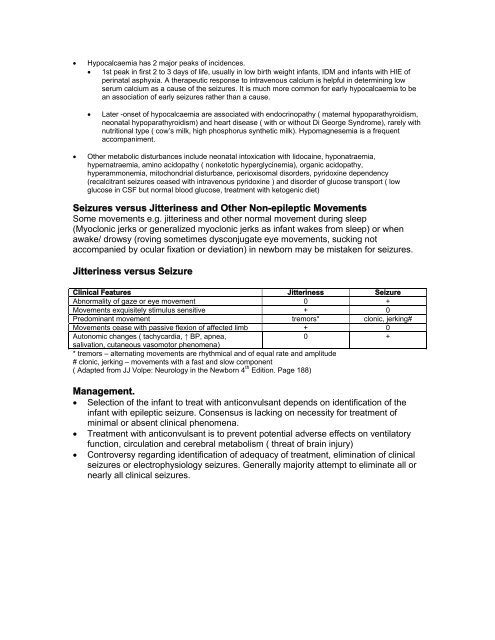
Jitteriness versus Seizure<br />
Clinical Features Jitteriness Seizure<br />
Abnormality of gaze or eye movement 0 +<br />
Movements exquisitely stimulus sensitive + 0<br />
Predominant movement tremors* clonic, jerking#<br />
Movements cease with passive flexion of affected limb + 0<br />
Autonomic changes ( tachycardia, ↑ BP, apnea,<br />
0 +<br />
salivation, cutaneous vasomotor phenomena)<br />
* tremors – alternating movements are rhythmical and of equal rate and amplitude<br />
# clonic, jerking – movements with a fast and slow component<br />
( Adapted from JJ Volpe: Neurology in the Newborn 4 th Edition. <strong>Page</strong> 188)<br />
Management.<br />
Selection of the infant to treat with anticonvulsant depends on identification of the<br />
infant with epileptic seizure. Consensus is lacking on necessity for treatment of<br />
minimal or absent clinical phenomena.<br />
Treatment with anticonvulsant is to prevent potential adverse effects on ventilatory<br />
function, circulation and cerebral metabolism ( threat of brain injury)<br />
Controversy regarding identification of adequacy of treatment, elimination of clinical<br />
seizures or electrophysiology seizures. Generally majority attempt to eliminate all or<br />
nearly all clinical seizures.













