

World Hospitals and Health Services - International Hospital ...
World Hospitals and Health Services - International Hospital ...
World Hospitals and Health Services - International Hospital ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
POLICY: PUBLIC HEALTH RESEARCH<br />
Causes of the problem at global level<br />
The global agenda has for too long neglected the diseases<br />
affecting the poor populations. Malaria research has just<br />
started to receive its due recognition after decades of despair<br />
in the period 1960s <strong>and</strong> 1980s although it still receives<br />
comparatively low funding compared to the size of the<br />
problem. Michaud <strong>and</strong> Murray (1996) estimated that the<br />
global expenditure on research for HIV/AIDS <strong>and</strong> asthma<br />
was, respectively, US$952 million <strong>and</strong> US$143 million,<br />
whereas for malaria <strong>and</strong> tuberculosis it was about 15- <strong>and</strong> 5-<br />
fold less at US$60 million <strong>and</strong> US$26 million respectively.<br />
Taking cancer as an example, the UK expenditure is about<br />
US$225 million, equivalent to US$1,525 per single UK<br />
cancer death (Anderson et al, 1996). Malaria, on the<br />
contrary, has global expenditure of the order of US$65 per<br />
single death, while it is responsible for a much higher death<br />
toll. Priority setting at the global level has not yet involved<br />
sufficiently for the developing world’s voice to have a strong<br />
focus on the causes of the greater global burden.<br />
The facilities for generating powerful scientists are lacking<br />
in the developing world due to historical reasons, <strong>and</strong> the<br />
tendency not to invest for the creation of infrastructure in<br />
the developing world is still a major stumbling block. Many<br />
funding agencies do not allow the inclusion of capacity<br />
building in developing countries in proposals seeking funds<br />
for public health research. It is difficult to persuade<br />
development agencies to allow for the inclusion of a research<br />
component when obviously the success of development<br />
projects depends on good data <strong>and</strong> monitoring processes.<br />
There is a glaring lack of strong training institutions for<br />
tropical medicine, low production of medical doctors <strong>and</strong><br />
other scientists in biomedical fields.<br />
The brain drain from developing countries continues<br />
thrive, even when we are aware of the negative<br />
consequences <strong>and</strong> there are no policies to halt it.<br />
Causes of the problem at regional level<br />
At the regional level, there is lack of strong research<br />
advocacy <strong>and</strong> coordination. Such mechanisms either do not<br />
exist or, as in Africa, have just been started <strong>and</strong> are still<br />
struggling to get on their feet. A few developing countries<br />
like India, Brazil <strong>and</strong> China have moved faster forward,<br />
because they rectified this anomaly earlier on.<br />
Consequently, there is little advocacy for political support<br />
<strong>and</strong> financial support by regional economic bodies.<br />
Funding mechanisms are lacking or poor, leading to little<br />
sense of ownership of the research agenda <strong>and</strong> of strategies<br />
for capacity building. It is not right that Africa has no<br />
common research funding mechanism similar to Europe or<br />
America. It is even unethical, given the huge disease burden.<br />
Regional priority setting is absent <strong>and</strong> regions have little<br />
influence on the global agenda. Networking at the regional<br />
level is especially poor <strong>and</strong> uncoordinated in Africa,<br />
resulting in poor research output – unlike the PAHO region<br />
<strong>and</strong> India.<br />
There is poor development of peer review systems,<br />
research monitoring <strong>and</strong> control bodies, leaving developing<br />
countries as sites to be used for sample <strong>and</strong> data collection<br />
for developed world laboratories, rather than being equal<br />
partners in research.<br />
Causes of the problem at national levels<br />
At the country level there is also weak research coordination,<br />
advocacy <strong>and</strong> promotion, leading to poor quality or lack of<br />
research prioritisation. Only a few countries in Africa have<br />
well-functioning national health research mechanisms. The<br />
industrial base is lacking <strong>and</strong> product development efforts<br />
linking research <strong>and</strong> industry are rare. National guidelines for<br />
partnership are lacking <strong>and</strong> ethical review bodies are weak or<br />
inexistent. Research funding is negligible <strong>and</strong> mechanisms to<br />
facilitate research to implementation are missing.<br />
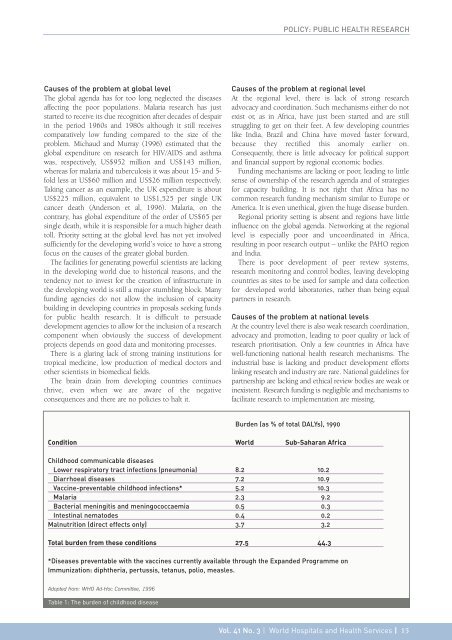
Burden (as % of total DALYs), 1990<br />
Condition <strong>World</strong> Sub-Saharan Africa<br />
Childhood communicable diseases<br />
Lower respiratory tract infections (pneumonia) 8.2 10.2<br />
Diarrhoeal diseases 7.2 10.9<br />
Vaccine-preventable childhood infections* 5.2 10.3<br />
Malaria 2.3 9.2<br />
Bacterial meningitis <strong>and</strong> meningococcaemia 0.5 0.3<br />
Intestinal nematodes 0.4 0.2<br />
Malnutrition (direct effects only) 3.7 3.2<br />
Total burden from these conditions 27.5 44.3<br />
*Diseases preventable with the vaccines currently available through the Exp<strong>and</strong>ed Programme on<br />
Immunization: diphtheria, pertussis, tetanus, polio, measles.<br />
Adopted from: WHO Ad-Hoc Committee, 1996<br />
Table 1: The burden of childhood disease<br />
Vol. 41 No. 3 | <strong>World</strong> <strong><strong>Hospital</strong>s</strong> <strong>and</strong> <strong>Health</strong> <strong>Services</strong> | 15














