Screening for cancer: are biomarkers of value?
Screening for cancer: are biomarkers of value?
Screening for cancer: are biomarkers of value?

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
– February/March 2011 22 Tumour markers<br />
Role <strong>of</strong> PSA iso<strong>for</strong>ms in improving<br />
PSA specificity in asymptomatic men<br />
An overview <strong>of</strong> the European Randomised Study <strong>of</strong> <strong>Screening</strong> <strong>for</strong><br />
Prostate Cancer (ERSPC) side studies indicates that biomarker panels<br />
would enhance accuracy <strong>of</strong> PCa screening in asymptomatic men [1].<br />
by Dr Chris Bangma<br />
The diagnosis <strong>of</strong> prostate <strong>cancer</strong> (PCa)<br />
continues to challenge both clinicians<br />
and their laboratory colleagues. With<br />
the incidence <strong>of</strong> PCa rising progressively<br />
each year, it is now the most common<br />
<strong>for</strong>m <strong>of</strong> malignancy amongst men<br />
in Europe. [2]. Prostate-specific antigen<br />
(PSA) has been the main driver <strong>for</strong> early<br />
detection <strong>of</strong> prostate <strong>cancer</strong>. Increasingly,<br />
over the last decade, we have seen how<br />
aw<strong>are</strong>ness <strong>of</strong> the PSA test has generated a<br />
storm <strong>of</strong> diagnostic activity, particularly in<br />
countries like the US, even in men with few<br />
or no symptoms.<br />
This tumour marker has attracted extraordinary<br />
scientific attention regarding its<br />
biochemical characteristics, epidemiological<br />
and clinical <strong>value</strong>, alongside huge<br />
commercial interest and increasing debate,<br />
even in the lay press [3, 4]. The level <strong>of</strong><br />
PSA at initial screening is highly indicative<br />
<strong>of</strong> PCa being diagnosed later in life<br />
– however, approximately half <strong>of</strong> <strong>cancer</strong>s<br />
detected in this way <strong>are</strong> found to be indolent<br />
[5]. It has always been recognised that<br />
many prostate <strong>cancer</strong> patients died with,<br />
rather than because <strong>of</strong>, their disease, but<br />
it was not <strong>for</strong>eseen that the impact <strong>of</strong> PSA<br />
screening <strong>of</strong> asymptomatic men would<br />
result in such a large number <strong>of</strong> indolent<br />
(slow growing) <strong>cancer</strong>s being detected.<br />
The ERSPC believes that the benefits <strong>of</strong><br />
screening would be significantly increased<br />
by the introduction <strong>of</strong> new <strong>biomarkers</strong><br />
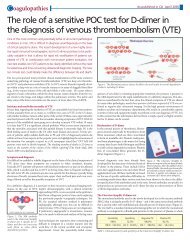
such as PSA iso<strong>for</strong>ms [Figure 1], and<br />
Complexed PSA<br />
Total PSA<br />
Other<br />
inactive<br />
PSA<br />
Truncated<br />
proPSA<br />
Free PSA<br />
Figure 1. SA and PSA Iso<strong>for</strong>ms – overview.<br />
Adapted by Chris Bangma from original table<br />
published in European Journal <strong>of</strong> Cancer, Oct<br />
2010 [1].<br />
BPSA<br />
the subsequent development <strong>of</strong> a panel <strong>of</strong><br />
screening tests. The additional analysis it<br />
carried out <strong>of</strong> candidate markers provides<br />
early encouragement. So far, the most<br />
promising results have been obtained from<br />
the analysis <strong>of</strong> free PSA, proPSA, nicked<br />
PSA and hK2 [6]. The availability <strong>of</strong> a<br />
panel <strong>of</strong> such markers could increase the<br />
specificity and sensitivity <strong>of</strong> screening <strong>for</strong><br />
prostate <strong>cancer</strong>, enabling new strategies to<br />
be developed <strong>for</strong> monitoring and asessing<br />
patient risk. This would reduce unnecessary<br />
biopsies, with surgical intervention<br />
only <strong>of</strong>fered to men at the highest risk.<br />
The first breakthrough in assessing the<br />
effectiveness <strong>of</strong> PSA testing on PCa mortality<br />
assessment came in March 2009 with the<br />
publication <strong>of</strong> the ERSPC study (involving<br />
an overall follow-up <strong>of</strong> up to 12 years) [7].<br />
It reported an initial reduction <strong>of</strong> at least<br />
20% in mortality, which rose to approximately<br />
30% when adjustment was made <strong>for</strong><br />
non-attendance <strong>of</strong> men enrolled in the<br />
study [8].<br />
Solving the dilemma <strong>of</strong><br />
overdiagnosis<br />
The likelihood <strong>of</strong> being diagnosed with prostate<br />
<strong>cancer</strong> in later life is highly dependent<br />
on the level <strong>of</strong> PSA at initial screening. PSA<br />
increases more quickly over time in men who<br />
get detectable <strong>cancer</strong>. However, the ERSPC<br />
study highlighted the serious limitations <strong>of</strong><br />
current PSA testing – that <strong>of</strong> overdiagnosis.<br />
In order to save one life, 1410 men would<br />
have to be tested and 48 men diagnosed with<br />
prostate <strong>cancer</strong>. To achieve this, an unacceptably<br />
high number <strong>of</strong> biopsies would<br />
subsequently be found to be negative.<br />
Current clinical practice uses a serum PSA<br />
<strong>value</strong> <strong>of</strong> more than 4 ng/mL to indicate<br />
abnormality; this is likely to lead to a prostatic<br />
biopsy. The case is less clear cut with<br />
men with a serum PSA between 2-4ng/mL.<br />
After undergoing a biopsy, 20 -30% <strong>of</strong> these<br />
men will be seen to have PCa, and <strong>of</strong> those,<br />
approximately one third <strong>of</strong> these <strong>cancer</strong>s<br />
<strong>are</strong> indolent and unlikely to cause death [9].<br />
Many patients have there<strong>for</strong>e undergone an<br />
unnecessary, invasive procedure– at a cost<br />
to both the men themselves and the health<br />
service involved. Based on the annual incidence,<br />
it is estimated that the annual number<br />
<strong>of</strong> unnecessary biopsies is around 750,000 in<br />
the US alone [10, 11].<br />
Throughout the duration <strong>of</strong> the study, the<br />
eight ERSPC countries involved used total<br />
PSA <strong>value</strong> as the sole indicator <strong>for</strong> biopsies.<br />
However, the study involved such a large<br />
sample (182,000 participants initially) that it<br />
was possible to carry out a number <strong>of</strong> additional<br />
country-specific studies specifically<br />
focusing on different candidate markers.<br />
Alongside evaluating changes in PSA concentrations<br />
over time (PSA velocity, PSA<br />
doubling), various PSA-iso<strong>for</strong>ms, kallikreins<br />
and molecular markers were assessed retrospectively<br />
in different ERSPC cohorts <strong>of</strong> men<br />
both with and without prostate <strong>cancer</strong>. The<br />
objective was to see what additional in<strong>for</strong>mation<br />
these candidate markers could add to<br />
the total PSA result hopefully enabling more<br />
selective PCa screening models to be developed<br />
<strong>for</strong> asymptomatic men.<br />
PSA is a kallikrein-like serine protease (also<br />
known as kallikrein-related peptidase 3),<br />
which is cleaved into smaller fragments as<br />
part <strong>of</strong> its biological pr<strong>of</strong>ile. Family members<br />
include kallikrein-related peptidase 2 (hK2),<br />
which is genetically and structurally very<br />
similar to PSA and also primarily localised to<br />
the epithelial cells <strong>of</strong> the prostate. hK2 rapidly<br />
converts the inactive precursor <strong>for</strong>m <strong>of</strong> PSA,<br />
proPSA, to active PSA and appears to be more<br />
strongly associated with prostate tumours<br />
than total PSA, being highly expressed in<br />
poorly differentiated <strong>cancer</strong> cells.<br />
Candidate markers —<br />
a brief glimpse at the possibilities<br />
From the side studies, the most promising<br />
potential <strong>biomarkers</strong> included % free PSA<br />
and free PSA <strong>for</strong>ms (intact/nicked PSA<br />
and proPSA) and hK2 [6]. ProPSA is found<br />
in normal prostatic epithelium together<br />
with truncated <strong>for</strong>ms. Mikolajczyk et al.<br />
identified a clinically important <strong>for</strong>m, (-2)<br />
proPSA, containing 239 amino acids. This<br />
<strong>for</strong>m is found in prostate <strong>cancer</strong> tissue as<br />
well as serum [12]. Indications <strong>are</strong> that the