Screening for cancer: are biomarkers of value?
Screening for cancer: are biomarkers of value?
Screening for cancer: are biomarkers of value?

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Weekly news updates on www.cli-online.com | February/March 2011 | Volume 35<br />
<strong>Screening</strong> <strong>for</strong> <strong>cancer</strong>:<br />
<strong>are</strong> <strong>biomarkers</strong> <strong>of</strong> <strong>value</strong>?<br />
Midkine ELISA<br />
Pg.06<br />
<br />
Pg.32<br />
Xylene-free<br />
tissue processing<br />
<br />
Pg.33<br />
Also in this issue :<br />
Immun<strong>of</strong>luorescence<br />
laboratory s<strong>of</strong>tw<strong>are</strong><br />
<br />
Pg.34<br />
Molecular <strong>for</strong>ms<br />
<strong>of</strong> PSA Pg. 14<br />
Serum free light chain<br />
analysis Pg. 18<br />
Genetic <strong>biomarkers</strong> in<br />
colorectal <strong>cancer</strong> Pg. 26
A Closer Look<br />
at Better Results<br />
Multi-Constituent Controls from the<br />
leader in oncology <strong>biomarkers</strong>.<br />
TUMOR MARKER<br />
ANALYTES<br />
HE4<br />
CA 15-3<br />
CA 19-9<br />
CA 125<br />
AFP<br />
CEA<br />
PSA<br />
FREE PSA<br />
FERRITIN<br />
From the company that brought you CA 125, CA 19-9, and CA 15-3, Fujirebio<br />
Diagnostics, Inc. now brings you a multi-constituent Tumor Marker Control. This<br />
quality control product contains clinically and medically relevant analyte levels.<br />
The Tumor Marker Control combines the per<strong>for</strong>mance levels you’d expect with<br />
the confi dence to release accurate, consistent patient results.<br />
K The only available multi-constituent control containing the novel biomarker HE4<br />
K Contains clinically relevant proportions <strong>of</strong> Free PSA and PSA-ACT<br />
K 100% human serum matrix, lyophilized, bi-level multi-constituent control<br />
K Reconstituted stability up to 60 days at ≤-20°C<br />
K Stable <strong>for</strong> up to nine freeze/thaw cycles<br />
K Web-based interQC real-time internal and external quality peer group reports<br />
CA 27.29*<br />
CA 242*<br />
* Non-spiked analytes. No claim is<br />
made <strong>for</strong> per<strong>for</strong>mance or stability.<br />
Look closer. Per<strong>for</strong>m better. Deliver more.<br />
FDI-264 04/10<br />
© 2010 Fujirebio Diagnostics, Inc. For more in<strong>for</strong>mation visit: www.fdimcc.com<br />
www.cli-online.com & search 25475<br />
C_CLI_ROW.indd 1 9/2/10 10:
Editor’s letter<br />
3<br />
– February/March 2011<br />
Prostate <strong>cancer</strong> management: a continuing challenge<br />
Accounting <strong>for</strong><br />
between 6 - 10 % <strong>of</strong><br />
<strong>cancer</strong> deaths in men,<br />
prostate <strong>cancer</strong> (PCa)<br />
is the second most<br />
frequently diagnosed<br />
<strong>cancer</strong> in the West,<br />
with around one in six<br />
men in the developed<br />
world eventually being diagnosed<br />
with the disease. While older age<br />
and family history increase the risk<br />
<strong>for</strong> PCa, there <strong>are</strong> no established<br />
modifiable risk factors; reduction<br />
in the mortality rate is dependent<br />
on early diagnosis and timely treatment.<br />
Although a routine blood test<br />
revealing an elevated prostate-specific<br />
antigen (PSA) level may detect<br />
PCa be<strong>for</strong>e symptoms have developed,<br />
despite its name this marker<br />
is actually far from specific. It may<br />
be elevated in several benign conditions,<br />
with the result being unnecessary<br />
biopsies. In addition, a considerable<br />
proportion <strong>of</strong> men with low<br />
levels <strong>of</strong> PSA below the cut-<strong>of</strong>f <strong>value</strong><br />
<strong>of</strong> 4 ng/mL actually have prostate<br />
<strong>cancer</strong>. Various research groups have<br />
thus been looking <strong>for</strong> more effective<br />
methods <strong>of</strong> measuring PSA as well<br />
as <strong>for</strong> more specific and sensitive<br />
markers <strong>for</strong> diagnosis and prognosis<br />
<strong>of</strong> the disease.<br />
Over the past decade several groups<br />
from prestigious institutes have<br />
reported that the use <strong>of</strong> prostatespecific<br />
antigen velocity (PSAV),<br />
which involves the change in PSA<br />
level over a specified time interval,<br />
is a more effective strategy <strong>for</strong> risk<br />
prediction, diagnosis and prognosis<br />
<strong>of</strong> PCa. Even in cases with total PSA<br />
levels below the cut-<strong>of</strong>f <strong>value</strong>, and<br />
certainly with <strong>value</strong>s between 4 and<br />
10 ng/mL, an elevated PSAV above<br />
0.4 ng/mL/year, has been reported<br />
to be a strong predictor <strong>of</strong> prostate<br />
<strong>cancer</strong> risk. An elevated PSAV was<br />
found to be significantly more likely<br />
to result in aggressive disease and<br />
ultimately death from PCa.<br />
However a recent comprehensive<br />
US study, reported in the Journal <strong>of</strong><br />
the National Cancer Institute and<br />
involving 5,000 men, found that<br />
even a rapid increase in PSA level<br />
was not necessarily linked to prostate<br />
<strong>cancer</strong> if the actual absolute<br />
level <strong>of</strong> the antigen was low. The<br />
researchers concluded that the<br />
PSA level varies naturally over<br />
time, so that men whose PSA level<br />
suddenly increases should have a<br />
repeat test rather than undergo a<br />
possibly unnecessary biopsy.<br />
However the controversy surrounding<br />
PSAV and its <strong>value</strong> in<br />
PCa screening can probably be<br />
explained by the fact that the many<br />
different PSA assays available <strong>are</strong><br />
not interchangeable, nor <strong>are</strong> they<br />
necessarily referenced to the same<br />
laboratory standards. To give reliable<br />
results, longitudinal monitoring<br />
<strong>of</strong> PSA must use the same assay<br />
and standard each time a subject is<br />
tested. Such individual risk assessment<br />
based on the doubling time<br />
www.partec.com<br />
<strong>of</strong> relevant markers, as well as the<br />
development <strong>of</strong> a panel <strong>of</strong> <strong>biomarkers</strong><br />
incorporating PSA iso<strong>for</strong>ms,<br />
will hopefully not only reduce<br />
unnecessary biopsies, but will have<br />
a significant impact on the overall<br />
prostate <strong>cancer</strong> mortality rate.<br />
Flow Cytometry |<br />
Cell Analysis | Diagnostics<br />
Applications<br />
Healthc<strong>are</strong><br />
Immunology<br />
HIV/AIDS, Malaria, TB<br />
Hematology, Pathology<br />
Cancer Research<br />
DNA Analysis<br />
CyFlow ® Flow Cytometry Systems<br />
Microbiology<br />
Cell Counting & Sorting<br />
Yeast/Bacteria/Viruses<br />
Live/Dead Analysis<br />
Toxicology<br />
Aquatic Sciences<br />
CyScope ®<br />
Fluorescence and<br />
Transmitted Light<br />
Microscopes<br />
Industry<br />
Quality Control in Food<br />
and Beverage Industry<br />
Pharmaceutical Industry<br />
Cosmetics Industry<br />
Biomonitoring<br />
mAbs &<br />
Reagents<br />
CyFox ®<br />
Real-Time „All in one“<br />
Gel Electrophoresis<br />
System<br />
Agrosciences<br />
Ploidy Analysis<br />
DNA Analysis<br />
Detection <strong>of</strong> Hybrids<br />
Cell Type Identification in<br />
Natural Populations<br />
Contact<br />
Partec GmbH | Am Flugplatz 13 | D-02828 Görlitz | Germany | Fon +49 3581 8746-0 | Fax +49 3581 8746-70 | mail@partec.com<br />
www.cyclos-design.de 03.11<br />
www.cli-online.com & search 25450
Contents<br />
FRONT COVER<br />
Midkine ELISA<br />
Xylene-free<br />
tissue processing<br />
Immun<strong>of</strong>l uorescence<br />
laboratory s<strong>of</strong>tw<strong>are</strong><br />
Pg.32<br />
Pg.33<br />
Pg.34<br />
FEATURES<br />
Weekly news updates on www.cli-online.com | February/March 2011 | Volume 35<br />
<strong>Screening</strong> <strong>for</strong> <strong>cancer</strong>:<br />
<strong>are</strong> <strong>biomarkers</strong> <strong>of</strong> <strong>value</strong>?<br />
Also in this issue :<br />
Molecular <strong>for</strong>ms Serum free light chain<br />
<strong>of</strong> PSA Pg. 14 analysis Pg. 18<br />
Pg.06<br />
Genetic <strong>biomarkers</strong> in<br />
colorectal <strong>cancer</strong> Pg. 26<br />
[6 - 8] <strong>Screening</strong> <strong>for</strong> <strong>cancer</strong>: <strong>are</strong> <strong>biomarkers</strong> <strong>of</strong> <strong>value</strong>?<br />
[10 - 12] Hybrid muliplex assays <strong>for</strong> the early detection<br />
<strong>of</strong> colorectal <strong>cancer</strong><br />
Intuitively, the measurement <strong>of</strong> <strong>biomarkers</strong> <strong>for</strong><br />
<strong>cancer</strong> screening has great appeal. However,<br />
those markers which have been most widely<br />
studied <strong>for</strong> <strong>cancer</strong> screening have been disappointing<br />
as regards reducing mortality from<br />
<strong>cancer</strong>, especially in asymptomatic populations.<br />
The real utility <strong>of</strong> <strong>biomarkers</strong> in screening looks<br />
more likely to be in high-risk populations, where<br />
the prevalence <strong>of</strong> <strong>cancer</strong> is high. One example<br />
<strong>of</strong> this is the use <strong>of</strong> human chorionic gonadotropin<br />
<strong>for</strong> screening <strong>for</strong> gestational trophoblastic<br />
neoplasia in patients who have had a previous<br />
diagnosis <strong>of</strong> a hydatidi<strong>for</strong>m mole.<br />
Rue Royale 326 • 1030 Brussels, Belgium<br />
Tel. +32-2-240 26 11 • Fax: +32-2-240 26 18<br />
www.cli-online.com<br />
Managing Editors<br />
Frances Bushrod, Ph.D.<br />
f.bushrod@panglobal.be<br />
Alan Barclay, Ph.D.<br />
Editorial Coordinator<br />
Anna Hyrkäs, M.Sc.<br />
Advertising Coordinator<br />
Jennifer Christophers<br />
Circulation Manager<br />
Arthur Léger<br />
Publisher<br />
Bernard Léger, M.D.<br />
Advertising Sales Manager<br />
Astrid Wydouw<br />
a.wydouw@panglobal.be<br />
Webmaster<br />
Damien Noël de Burlin<br />
©2011 by PanGlobal Media bvba-sprl. Production &<br />
Lay-out by Studiopress Communication, Brussels.<br />
Circulation Controlled by Business <strong>of</strong><br />
Per<strong>for</strong>ming Audits, Shelton, CT, USA.<br />
[14 - 16] Clinical and analytical implications <strong>of</strong> molecular<br />
<strong>for</strong>ms <strong>of</strong> PSA in serum<br />
[18 - 20] Myeloma screening: an update<br />
The publisher assumes no responsibility <strong>for</strong> opinions or statements<br />
expressed in advertisements or product news items.<br />
The opinions expressed in by-lined articles <strong>are</strong> those <strong>of</strong> the<br />
author and do not necessarily reflect those <strong>of</strong> the publisher. No<br />
conclusion can be drawn from the use <strong>of</strong> trade marks in this<br />
publication as to whether they <strong>are</strong> registered or not.<br />
ISSN 1373-1580<br />
Coming up in<br />
April/May 2011<br />
[22 - 24] An overview <strong>of</strong> the ERSPC side studies and prostate <strong>cancer</strong><br />
[26 - 28] Genetic <strong>biomarkers</strong> in colorectal <strong>cancer</strong><br />
[29 - 30] Indirect detection methods <strong>for</strong> syphilis diagnosis<br />
Respiratory focus<br />
Immunodiagnostics<br />
For submission <strong>of</strong> editorial material, contact<br />
Frances Bushrod at f.bushrod@panglobal.be<br />
For advertising in<strong>for</strong>mation, go online to<br />
www.cli-online.com, simply click on ‘Magazine’<br />
and ‘Media In<strong>for</strong>mation’ or contact<br />
Astrid Wydouw at a.wydouw@panglobal.be<br />
REGULARS<br />
[3] Editor’s letter<br />
[25] News in brief<br />
[31 - 34] Product news<br />
Free Subscription <strong>for</strong><br />
Clinical lab pr<strong>of</strong>essionals<br />
Clinical lab pr<strong>of</strong>essionals <strong>are</strong> entitled to receive the<br />
digital edition <strong>of</strong> CLI <strong>for</strong> the next 12 months completely<br />
free <strong>of</strong> charge. To begin a new subscription<br />
or to continue your existing free subscription go to<br />
www.cli-online.com<br />
Click on Free Subscription and follow instructions
www.smartautomation.eu<br />
www.smartautomation.eu<br />
www.cli-online.com & search 25358<br />
11-010-SFE-Adv CLI febr-mrt-188x276-v3.indd 1 1-3-11 11:11
– February/March 2011 6 Tumour markers<br />
<strong>Screening</strong> <strong>for</strong> <strong>cancer</strong>:<br />
<strong>are</strong> <strong>biomarkers</strong> <strong>of</strong> <strong>value</strong>?<br />
Intuitively, the measurement <strong>of</strong> <strong>biomarkers</strong> <strong>for</strong> <strong>cancer</strong> screening has<br />
great appeal. This article reviews the current status <strong>of</strong> the <strong>biomarkers</strong><br />
most widely studied in <strong>cancer</strong> screening, but concludes that their use<br />
to date has been disappointing in reducing mortality from <strong>cancer</strong>,<br />
especially in asymptomatic populations. Their main utility in screening<br />
is likely to be in high-risk populations, where the prevalence <strong>of</strong> <strong>cancer</strong><br />
is high. An example is the use <strong>of</strong> human chorionic gonadotropin<br />
<strong>for</strong> screening <strong>for</strong> gestational trophoblastic neoplasia in patients<br />
who have had a previous diagnosis <strong>of</strong> a hydatidi<strong>for</strong>m mole.<br />
by Pr<strong>of</strong>. Michael J Duffy<br />
<strong>Screening</strong> <strong>for</strong> <strong>cancer</strong> has great intuitive appeal,<br />
since it is widely believed that the early detection<br />
<strong>of</strong> malignancy followed by the initiation<br />
<strong>of</strong> treatment results in improved outcome.<br />
Consequently, population-based screening<br />
<strong>for</strong> different types <strong>of</strong> <strong>cancer</strong> is now available<br />
in many countries, including mammography<br />
<strong>for</strong> breast <strong>cancer</strong> in women over 50 years <strong>of</strong><br />
age, the PAP smear <strong>for</strong> cervical <strong>cancer</strong> and<br />
either colonoscopy or faecal occult blood<br />
testing (FOBT) <strong>for</strong> colorectal <strong>cancer</strong>.<br />
Comp<strong>are</strong>d to procedures such as mammography,<br />
colonoscopy and smear testing, the<br />
measurement <strong>of</strong> <strong>biomarkers</strong> is considerably<br />
simpler and more convenient [1]. However,<br />
as previously pointed out by Dr Sturgeon [3],<br />
<strong>biomarkers</strong> generally have low sensitivities<br />
and low specificities <strong>for</strong> early malignancy.<br />
These disadvantages, when combined with<br />
the low prevalence <strong>of</strong> <strong>cancer</strong>s in a healthy<br />
population, greatly limit the use <strong>of</strong> <strong>biomarkers</strong><br />
in screening programmes, especially<br />
when used alone. Despite these disadvantages,<br />
several <strong>biomarkers</strong> have either undergone<br />
or <strong>are</strong> currently undergoing investigation<br />
<strong>for</strong> <strong>cancer</strong> screening [Table 1]. The aim<br />
<strong>of</strong> this article is to briefly review the current<br />
status <strong>of</strong> the <strong>biomarkers</strong> most widely<br />
studied <strong>for</strong> <strong>cancer</strong> screening.<br />
PSA in screening <strong>for</strong><br />
prostate <strong>cancer</strong><br />
Although ad hoc or opportunistic screening<br />
<strong>for</strong> prostate <strong>cancer</strong> is now common, the<br />
benefit <strong>of</strong> this is unclear. Ideally, prior to<br />
being used in general population screening,<br />
a new screening modality should be shown<br />
to reduce disease-specific mortality in a<br />
large prospective randomised trial. In 2009,<br />
preliminary results from two such trials on<br />
prostate <strong>cancer</strong> screening were published.<br />
One <strong>of</strong> these trials, the European Randomised<br />
Study <strong>of</strong> prostate Cancer (ERSPC)<br />
[4], was carried out in seven European<br />
countries, while the second, known as the<br />
Prostate, Lung, Colon and Ovary (PLCO)<br />
trial [5] was per<strong>for</strong>med in the USA. After<br />
7-10 years <strong>of</strong> follow-up in this study, similar<br />
rates <strong>of</strong> death from prostate <strong>cancer</strong> were<br />
found in the screened and control arm. This<br />
trial however, had several flaws including a<br />
high frequency <strong>of</strong> PSA testing prior to the<br />
start <strong>of</strong> the trial and substantial contamination<br />
<strong>of</strong> the control group (i.e., subjects in the<br />
control group had high rates <strong>of</strong> PSA testing).<br />
Furthermore, there was a low rate <strong>of</strong><br />
diagnostic biopsies in subjects with elevated<br />
PSA levels during the trial.<br />
Comp<strong>are</strong>d to the PLCO trial, the European<br />
study had a greater number <strong>of</strong> participating<br />
subjects, longer follow-up and less contamination<br />
<strong>of</strong> the control arm. Although<br />
Marker or test<br />
it showed that screening resulted in a 20%<br />
reduction in mortality, the authors calculated<br />
that 1410 men would have to be<br />
screened and 48 additional cases <strong>of</strong> prostate<br />
<strong>cancer</strong> would have to undergo treatment to<br />
prevent one death from prostate <strong>cancer</strong> [4].<br />
With these conflicting findings, it is not<br />
surprising that published guidelines on<br />
prostate <strong>cancer</strong> screening differ in their<br />
recommendations as to whether or not<br />
asymptomatic men should undergo PSA<br />
testing <strong>for</strong> prostate <strong>cancer</strong> [6]. Although<br />
expert panels differ in their recommendations<br />
regarding PSA screening, most state<br />
that prior to any testing, men should be<br />
counselled regarding potential risks and<br />
benefits <strong>of</strong> screening and that a sh<strong>are</strong>d<br />
approach to decision making between<br />
doctor and patient should occur.<br />
Faecal Occult Blood Testing<br />
in screening <strong>for</strong> colorectal <strong>cancer</strong><br />
In contrast to the role <strong>of</strong> PSA in prostate<br />
<strong>cancer</strong> screening, four large randomised<br />
prospective trials have all shown that<br />
screening app<strong>are</strong>ntly healthy subjects over<br />
50 years <strong>of</strong> age using FOBT reduces mortality<br />
from CRC [7]. Combined results from<br />
the four trials showed that the screening<br />
resulted in a 16% reduction in the relative<br />
risk <strong>of</strong> CRC mortality [7]. Following adjustment<br />
<strong>for</strong> those subjects that failed to attend<br />
screening, mortality reduction increased to<br />
25%. Combined results from the four trials<br />
however, failed to show a significant difference<br />
in all-cause mortality between the<br />
screened and control groups. This failure<br />
Malignancy<br />
Effect on reducing<br />
mortality<br />
FOBT Colorectal Yes<br />
PSA Prostate Unclear<br />
CA 125 Ovarian Unclear<br />
AFP Hepatocellular* Yes**<br />
VMA/HVA Neuroblastoma No<br />
Pepsinogen Stomach* Unclear<br />
HCG Trophoblastic*** Yes<br />
Table 1. Biomarkers that have undergone or <strong>are</strong> currently undergoing evaluation in screening <strong>for</strong><br />
<strong>cancer</strong>. *Only in high-risk <strong>are</strong>as/high risk subjects. **Shown in a randomised trial to reduce mortality<br />
in high-risk subjects in China (2). ***In patients who have had a previous hydatidi<strong>for</strong>m mole.
7<br />
– February/March 2011<br />
to show a reduction in all-cause mortality<br />
is likely to be due the fact that mortality<br />
from CRC made a relatively low contribution<br />
to overall mortality. Nevertheless,<br />
based on the above results, pilot or regional<br />
CRC screening trials have now commenced<br />
in several countries and <strong>are</strong> under<br />
consideration in several others.<br />
The FOBT used in the above randomised trials<br />
was per<strong>for</strong>med with the guaiac test which<br />
relies on the pseudo peroxidase activity <strong>of</strong><br />
haem, either as intact haemoglobin or free<br />
haem. The guaiac FOBT (gFOBT) system<br />
however, has several limitations such as lack<br />
<strong>of</strong> specificity <strong>for</strong> human haemoglobin (certain<br />
foodstuffs and medications may interfere<br />
with the test) and relatively low clinical sensitivity<br />
and specificity <strong>for</strong> colorectal neoplasia<br />
[8]. In addition, it is difficult to automate,<br />
making it unsuitable <strong>for</strong> population-based<br />
screening [8].<br />
In an attempt to overcome some <strong>of</strong> these<br />
limitations, the faecal immunochemical test<br />
(FIT) was introduced. This test specifically<br />
detects the globin component <strong>of</strong> haemoglobin<br />
in an immunochemical assay. Some<br />
<strong>of</strong> the main advantages <strong>of</strong> FITs over gFOBTs<br />
<strong>are</strong> summarised in Table 2. Because <strong>of</strong> these<br />
advantages, European Group on Tumor<br />
Markers expert panel recently recommended<br />
use <strong>of</strong> a FIT <strong>for</strong> the new centres embarking<br />
on FOBT screening <strong>for</strong> CRC [8].<br />
AFP in screening <strong>for</strong><br />
hepatocellular <strong>cancer</strong><br />
The incidence <strong>of</strong> hepatocellular <strong>cancer</strong><br />
(HCC) varies widely throughout the world,<br />
being highest in South-East Asia and Sub-<br />
Saharan Africa and relatively low in Europe<br />
and North America [9]. Its incidence in the<br />
West however, has increased in recent years,<br />
mainly due to infection with the hepatitis<br />
C virus. The most important risk factor <strong>for</strong><br />
HCC is liver cirrhosis which most commonly<br />
results from infection with hepatitis<br />
B or C virus, or high intake <strong>of</strong> alcohol. Since<br />
groups at high risk <strong>of</strong> developing HCC can be<br />
identified, screening had been advocated <strong>for</strong><br />
detecting early malignancy in these subjects.<br />
The biomarker most widely used in screening<br />
<strong>for</strong> HCC is AFP. However, as AFP lacks<br />
sensitivity <strong>for</strong> early disease, it is usually<br />
combined with abdominal ultrasound<br />
(US) in screening <strong>for</strong> HCC. Thus, the<br />
National Academy <strong>of</strong> Clinical Biochemistry<br />
(NACB) [10] recommends that both AFP<br />
and abdominal US be per<strong>for</strong>med at sixmonthly<br />
intervals in patients at high risk<br />
<strong>of</strong> HCC, especially those with hepatitis B<br />
and hepatitis C-related liver cirrhosis. The<br />
NACB also state that “AFP concentrations<br />
that <strong>are</strong> >20 µg/L and increasing should<br />
prompt further investigation, even if US<br />
is negative” [10]. Similarly, the National<br />
Comprehensive Cancer Network (NCCN)<br />
recommends ultrasound and measurement<br />
<strong>of</strong> AFP every six months to screen<br />
high risk subjects <strong>for</strong> HCC. This organisation<br />
also recommends additional imaging,<br />
such as contrast CT if AFP levels <strong>are</strong> rising,<br />
or following identification <strong>of</strong> a liver mass<br />
nodule on ultrasound [11]. In contrast<br />
to the NACB and NCCN, the American<br />
Association <strong>for</strong> the Study <strong>of</strong> Liver Disease<br />
(AASLD) recommends that AFP should<br />
not be used in the surveillance <strong>of</strong> highrisk<br />
groups <strong>for</strong> HCC unless ultrasound<br />
is unavailable [12]. New guidelines <strong>for</strong>m<br />
the AASLD however, do not include AFP<br />
determination in their recommendations<br />
<strong>for</strong> HCC screening (http://www.aasld.org/<br />
practiceguidelines/Pages/NewUpdated-<br />
Guidelines.aspx).<br />
CA 125 in screening <strong>for</strong><br />
ovarian <strong>cancer</strong><br />
Comp<strong>are</strong>d to the <strong>cancer</strong>s discussed above,<br />
ovarian <strong>cancer</strong> is relatively r<strong>are</strong>, with an<br />
incidence rate <strong>of</strong> approximately one in 70<br />
women [13]. Although relatively r<strong>are</strong>, ovarian<br />
<strong>cancer</strong> is the 4 th most common cause<br />
<strong>of</strong> <strong>cancer</strong>-related death in women and the<br />
most lethal gynaecological malignancy.<br />
The high death rate, at least in part, reflects<br />
the fact that most women with ovarian<br />
<strong>cancer</strong> <strong>are</strong> diagnosed at an advanced stage,<br />
i.e., 65-75% <strong>of</strong> women with ovarian <strong>cancer</strong>s<br />
have stage III/IV disease at diagnosis. The<br />
5-year survival rate <strong>for</strong> these patients is<br />
only about 20%-30%. On the other hand,<br />
Confidence<br />
in results<br />
Quality Assurance Scheme<br />
Join the 300 laboratories<br />
worldwide who quality assure<br />
their Freelite TM serum free light<br />
chains assays with IMMPROVE<br />
Serum Paraprotein scheme<br />
QA003.<br />
• Quality assure your quantitative<br />
results <strong>for</strong>:<br />
IgG, IgA, IgM<br />
B2 microglobulin<br />
Freelite free kappa<br />
Freelite free lambda<br />
Freelite free kappa/lambda ratio<br />
• Enjoy speedy result submission<br />
via secure website<br />
• Confidence assured with a<br />
comprehensive report <strong>for</strong><br />
specific method, overall<br />
statistics & expert opinion<br />
For more in<strong>for</strong>mation contact us at<br />
Immprove@bindingsite.co.uk<br />
or visit our website at<br />
www.bindingsite.com/paraproteinqa-scheme<br />
IMMPROVE TM and Freelite TM <strong>are</strong> trademarks <strong>of</strong><br />
The Binding Site Group Ltd, Birmingham, UK.<br />
FITs have better analytical sensitivity and specificity <strong>for</strong> human haemoglobin than<br />
guaiac-based tests.<br />
Some FITs can be automated, thus increasing throughput and reproducibility.<br />
Some FITs can be quantitated, enabling adjustment <strong>of</strong> sensitivity, specificity and<br />
positivity rates to meet local needs.<br />
Unlike the guaiac tests which may be affected by certain dietary components<br />
(e.g., red meat, vitamin C) and some medications (e.g., aspirin), FITs <strong>are</strong> free<br />
from interference by these factors.<br />
Table 2. Advantages <strong>of</strong> the faecal immunochemical test (FIT) over the guaiac faecal occult blood<br />
testing (gFOBT). Data summarised from [8].<br />
The Binding Site Group Ltd<br />
Tel: +44 (0)121 456 9500<br />
info@bindingsite.co.uk<br />
www.bindingsite.com<br />
The Specialist Protein Company<br />
www.cli-online.com & search 25375
– February/March 2011 8 Tumour markers<br />
a 5-year survival rate <strong>of</strong> >90% can be<br />
achieved when disease is confined to the<br />
ovary. Un<strong>for</strong>tunately, only about 25% <strong>of</strong><br />
ovarian <strong>cancer</strong>s <strong>are</strong> detected at this early<br />
stage. This correlation between 5-year survival<br />
rates and stage at diagnosis suggests<br />
that screening and early detection may<br />
improve outcome.<br />
Because <strong>of</strong> its relatively low prevalence, a<br />
screening strategy <strong>for</strong> ovarian <strong>cancer</strong> must<br />
have an extremely high specificity to minimise<br />
the number <strong>of</strong> false-positive results.<br />
Based on a prevalence <strong>of</strong> 40 cases per<br />
100,000 women, it has been estimated that<br />
in order to achieve an acceptable positive<br />
predictive <strong>value</strong> (at least 10%), an ovarian<br />
<strong>cancer</strong> screening strategy should have a<br />
specificity <strong>of</strong> 99.6% [14].<br />
The main screening tests undergoing evaluation<br />
<strong>for</strong> ovarian <strong>cancer</strong> <strong>are</strong> CA 125 and<br />
transvaginal ultrasound (TVS). Currently,<br />
two large prospective trials <strong>are</strong> evaluating<br />
these modalities in screening healthy<br />
women <strong>for</strong> ovarian <strong>cancer</strong>, namely the<br />
PLCO study in the US [15] and the United<br />
Kingdom Collaborative Trial <strong>of</strong> Ovarian<br />
Cancer <strong>Screening</strong> (UKCTOCS) [16].<br />
Preliminary results from the UK trial <strong>are</strong><br />
promising. Thus, <strong>of</strong> the 58 <strong>cancer</strong>s detected<br />
with CA 125 and TVS, 28 (48%) were<br />
found to be either stage I or II. Sensitivity,<br />
specificity and PPV <strong>of</strong> the two tests <strong>for</strong><br />
primary and tubal malignancies combined<br />
were respectively 89.4%, 99.8% and 35.1%.<br />
Currently, it is unclear whether screening<br />
with CA 125 and TVS reduces mortality<br />
from ovarian <strong>cancer</strong> [16]. Guidelines<br />
there<strong>for</strong>e recommend against the use <strong>of</strong><br />
CA 125 either alone or in combination<br />
with TVS in screening <strong>for</strong> ovarian <strong>cancer</strong><br />
in asymptomatic average-risk women outside<br />
the context <strong>of</strong> a randomised controlled<br />
trial [6,17].<br />
HCG in screening <strong>for</strong> gestational<br />
tropohoblastic neoplasia<br />
Gestational trophoblastic neoplasia (GTN)<br />
is a r<strong>are</strong> malignancy that originates from<br />
placental tissue. Although most GTNs<br />
develop following a molar pregnancy, they<br />
can occur after any antecedent pregnancy.<br />
As previously pointed out [3,18], the use <strong>of</strong><br />
human chorionic gonadotropin (HCG) to<br />
screen <strong>for</strong> GTN in patients diagnosed with<br />
a hydatidi<strong>for</strong>m mole approaches the ideal<br />
use <strong>of</strong> a screening biomarker as:<br />
• HCG levels <strong>are</strong> increased in almost all<br />
patients with trophoblastic disease,<br />
• HCG is a highly sensitive marker <strong>for</strong><br />
small volume trophoblastic disease,<br />
• The prevalence <strong>of</strong> malignant trophoblastic<br />
disease in women diagnosed with a previous<br />
hydatidi<strong>for</strong>m mole is relatively high<br />
(3 to 15%) and<br />
• Effective chemotherapy is available <strong>for</strong><br />
malignant trophoblastic disease.<br />
The combination <strong>of</strong> HCG measurements,<br />
organised follow-up and availability <strong>of</strong><br />
effective chemotherapy means that GTN<br />
is one <strong>of</strong> a few human malignancies that is<br />
curable, even in advanced stages <strong>of</strong> the disease.<br />
Indeed, cure rates <strong>for</strong> this malignancy<br />
now approach 100%. An important practical<br />
point in measuring HCG in GTN is that the<br />
assay used should detect all the main <strong>for</strong>ms<br />
<strong>of</strong> the protein, especially the beta subunit.<br />
Conclusion<br />
Although the measurement <strong>of</strong> <strong>biomarkers</strong><br />
has great appeal <strong>for</strong> <strong>cancer</strong> screening,<br />
their use to date has been disappointing<br />
from the point <strong>of</strong> view <strong>of</strong> reducing mortality<br />
from <strong>cancer</strong>, especially in asymptomatic<br />
populations. Their main utility in screening<br />
is likely to be in high-risk populations,<br />
where the prevalence <strong>of</strong> <strong>cancer</strong> is high. A<br />
good example <strong>of</strong> this is the use <strong>of</strong> HCG in<br />
screening <strong>for</strong> GTN in patients who had a<br />
previous diagnosis <strong>of</strong> a hydatidi<strong>for</strong>m mole.<br />
References<br />
1. Duffy MJ. J Int Fed Clin Chem Lab Med (JIFCC)<br />
2010;21:issue 1.<br />
2. Zhang B-H, Yang B-H, Tang ZY. J Cancer Clin<br />
Oncol 2004;130:417-422.<br />
3. Sturgeon C. A wide role <strong>for</strong> tumour markers in<br />
screening. Clin Lab Int April 2006.<br />
4. Schröder FH, Hugosson J, Roobol MJ, et al. N Engl J<br />
Med 2009;26;360:1320-8.<br />
5. Andriole GL, Craw<strong>for</strong>d ED, Grubb RL 3rd, et al. N<br />
Engl J Med 2009;360:1310-9.<br />
6. Sturgeon CM, Duffy MJ, Stenman UK et al. Clin<br />
Chem 2008;54:e11-79.<br />
7. Hewitson P, Glasziou P, Irwig L, Towler B, Watson<br />
E. Cochrane Database <strong>of</strong> Systematic Reviews 2007,<br />
Issue 1, Art. No.: CD001216. DOI: 10.1002/14651858.<br />
CD001216.pub2.<br />
8. Duffy MJ, van Rossum LG, van Turenhout ST et al.<br />
Int J Cancer 2011;128:3-11.<br />
9. Parikh S, Hyman D. Am J Med 2007;120:194-202.<br />
10. Sturgeon CM, Duffy MJ, H<strong>of</strong>mann BR et al. Clin<br />
Chem 2010;56:e1-48.<br />
11. National Comprehensive Cancer Network<br />
(NCCN) Clinical Practice Guidelines in Oncology,<br />
Hepatobiliary Cancers Version 2. 2010. http://<br />
www.nccn.org/ (Accessed, 27 Jan, 2011).<br />
12. Bruix J, Sherman M. Hepatology 2005;42:1208-36.<br />
13. Clarke-Pearson DL. N Engl J Med 2009;361:170-176.<br />
14. Jacobs I, Bast RC. Human Reprod 1989;4:1-12.<br />
15. Buys SS, Partridge E, Greene MH et al. Am J Obstet<br />
Gynecol 2005;193:1630-1639.<br />
16. Menon U, Gentry-Maharaj A, Hallett R et al. Lancet<br />
Oncol 2009;10:327-40.<br />
17. Duffy MJ, Bonfrer JM, Kulpa J et al. Int J Gynecol<br />
Cancer 2005;15:679-691.<br />
18. Duffy MJ. Crit Rev Clin Lab Sci 2001;38:225-262.<br />
The author<br />
Michael J Duffy<br />
Dept <strong>of</strong> Pathology and Laboratory<br />
Medicine<br />
St Vincent’s University Hospital, Dublin 4,<br />
UCD School <strong>of</strong> Medicine and Medical Science,<br />
University College Dublin, Dublin 4, Ireland.<br />
Corresponding address:<br />
Pr<strong>of</strong>essor M J Duffy<br />
Dept <strong>of</strong> Pathology and Laboratory<br />
Medicine<br />
St Vincent’s University Hospital<br />
Elm Park, Dublin 4, Ireland.<br />
Tel. +353-1-2094378<br />
e-mail: michael.j.duffy@ucd.ie<br />
BioVitrum and Sakura Finetek<br />
Europe selected to modernise<br />
Russian oncology<br />
Over the period<br />
2009 to 2013 the<br />
Russian government<br />
is providing<br />
the Russian<br />
national Health<br />
Programme with a<br />
special budget <strong>of</strong> approximately e11 billion<br />
to be used in programmes aimed at<br />
modernising the country’s <strong>cancer</strong> healthc<strong>are</strong><br />
system. The main programme is split<br />
into different sub-programmes covering<br />
specific medical <strong>are</strong>as, such as <strong>cancer</strong><br />
research and oncology, with one aim<br />
<strong>of</strong> the sub-programmes being to equip<br />
a certain number <strong>of</strong> hospitals each year<br />
with the latest technology.<br />
Since 2009, BioVitrum, Sakura Finetek<br />
Europe’s exclusive distributor in Russia<br />
and the <strong>for</strong>mer CIS countries, has been<br />
granted over 70% <strong>of</strong> all issued public tenders<br />
in the oncology sub-programme and<br />
has modernised 14 hospitals nationwide<br />
through the installation <strong>of</strong> high-per<strong>for</strong>mance<br />
Tissue-Tek instruments. These hospitals<br />
<strong>are</strong> now providing excellent patient<br />
c<strong>are</strong> such as the reduction <strong>of</strong> both <strong>cancer</strong><br />
waiting times and misdiagnosis rates;<br />
this is achieved through the provision<br />
<strong>of</strong> a superior laboratory environment<br />
equipped with highly reliable and innovative<br />
instruments that improve the quality<br />
and efficiency <strong>of</strong> <strong>cancer</strong> diagnosis and<br />
treatment. As a result, patients <strong>are</strong> now<br />
able to get their diagnosis within one day.<br />
www.smartautomation.eu
Can my urinalysis system<br />
stretch to meet all my needs?<br />
New!<br />
CLINITEK Status Systems ensure flexible, seamless connectivity.<br />
Whether you’re in a physician’s <strong>of</strong>fice or the hospital point <strong>of</strong> c<strong>are</strong>, the CLINITEK Status® Connect System and<br />
CLINITEK Status®+ Analyzer connect you to all aspects <strong>of</strong> urinalysis testing. Advanced operational controls help reduce<br />
risk and drive compliance. And, as your connectivity needs change, Siemens future-ready portfolio has the flexibility to<br />
grow with you. Discover five reasons why you should choose Siemens urine analyzers at www.usa.siemens.com/clinitek<br />
Answers <strong>for</strong> life.<br />
A91DX-9109-A1-4A00<br />
© 2010 Siemens Healthc<strong>are</strong> Diagnostics Inc. All rights reserved.<br />
CLINITEK Status and all associated marks <strong>are</strong> trademarks <strong>of</strong> Siemens Healthc<strong>are</strong> Diagnostics Inc.<br />
www.cli-online.com & search 25417
– February/March 2011 10 Tumour markers<br />
Hybrid multiplex assays <strong>for</strong> the early<br />
detection <strong>of</strong> colorectal <strong>cancer</strong>:<br />
a perspective<br />
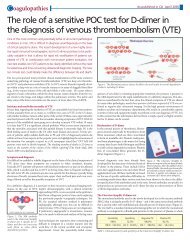
The early detection <strong>of</strong> colorectal <strong>cancer</strong> (CRC) is one <strong>of</strong> the great challenges in the<br />
battle against this disease. This article illustrates the power <strong>of</strong> immunoproteomic<br />
analysis <strong>of</strong> the serum antibody repertoire to pinpoint tumour-associated antigens<br />
directly from patient serum samples. Accumulating evidence indicates that<br />
certain intestinal bacteria can also play an important signalling function in CRC<br />
diagnostics. As the immune response against infectious agents is in general more<br />
pronounced than the response to altered self-proteins from tumour cells, antigens<br />
from an infectious agent could be instrumental in the immunodiagnosis <strong>of</strong> this<br />
disease. Eventually hybrid multimarker assays could be developed with a diagnostic<br />
accuracy that meets the stringent criteria <strong>for</strong> CRC screening at the population level.<br />
by Dr Harold Tjalsma<br />
The need <strong>for</strong> early<br />
detection <strong>of</strong> CRC<br />
Sporadic <strong>cancer</strong>s <strong>of</strong> the colon<br />
and rectum <strong>are</strong> the second<br />
most frequent malignancy in<br />
Western societies. Almost 1<br />
million cases occur annually<br />
worldwide, and nearly half<br />
a million patients die from<br />
CRC each year. About 45%<br />
<strong>of</strong> the cases <strong>are</strong> detected at<br />
an advanced stage, which is<br />
mainly because the flexibility <strong>of</strong><br />
the colon and its content allows<br />
relatively large tumours to be<br />
asymptomatic <strong>for</strong> a long time.<br />
Treatment is then difficult or<br />
even impossible, whereas early<br />
stage CRC can be effectively<br />
cured by surgical removal <strong>of</strong><br />
the diseased part <strong>of</strong> the colon<br />
[1,2]. Thus, the largest decrease<br />
in CRC mortality will probably<br />
not be achieved by better therapeutics,<br />
but by better tools <strong>for</strong><br />
CRC diagnosis at an early stage.<br />
Importantly, CRC progresses<br />
very slowly; the diagnostic<br />
window <strong>of</strong> opportunity may<br />
be as long as one decade [Figure<br />
1]. Faecal occult blood tests<br />
(FOBT) <strong>are</strong> <strong>of</strong>ten used nowadays<br />
to pre-select high-risk<br />
individuals <strong>for</strong> further colonoscopic<br />
evaluation. Among the<br />
weaknesses <strong>of</strong> the FOBT is its<br />
limited sensitivity, which is<br />
estimated to be around 50% <strong>for</strong><br />
tumours. Importantly, highrisk<br />
adenomas (polyps) <strong>are</strong><br />
Figure 1. Temporal response to bacterial & tumour antigens during<br />
CRC development.<br />
only detected in about 10-20%<br />
<strong>of</strong> cases as these <strong>are</strong> not <strong>of</strong>ten<br />
accompanied by intestinal<br />
bleedings [3]. Nevertheless, it is<br />
generally believed that screening<br />
the elderly (>50y) population<br />
<strong>for</strong> CRC would decrease<br />
morbidity and mortality. Thus,<br />
a simple and accurate screening<br />
assay is the holy grail in CRC<br />
diagnostics.<br />
Antigens as<br />
molecular markers<br />
An ideal molecular marker <strong>for</strong><br />
CRC should be one that is specifically<br />
produced by tumour<br />
cells, or is closely associated<br />
with diseased cells [4]. For<br />
clinical applications, blood is<br />
the body fluid <strong>of</strong> choice <strong>for</strong> biomarker<br />
assessment as homeostasis<br />
means its composition is<br />
normally stable. Immunoproteomic<br />
approaches take advantage<br />
<strong>of</strong> the fact that higher<br />
organisms have a sophisticated<br />
system to distinguish “normal”<br />
(self) from “abnormal” (nonself)<br />
proteins. In most cases,<br />
non-self proteins originate<br />
from invading fungi, parasites,<br />
bacteria and viruses, however,<br />
aberrant host proteins can<br />
also be recognised as non-self.<br />
In the latter case, the immune<br />
response is driven by abnormal<br />
expression <strong>of</strong> proteins or<br />
by molecular alterations, such<br />
as those resulting from mutations,<br />
misfolding, aberrant<br />
degradation, glycosylation<br />
or truncated frameshift peptides<br />
[4,5] that render these<br />
proteins immunogenic.<br />
For diagnostic purposes, several<br />
features <strong>of</strong> circulating antibodies<br />
<strong>are</strong> important: i) they<br />
reflect a molecular imprint <strong>of</strong><br />
disease-related antigens from<br />
the entire human body; ii)<br />
although an antigen may be<br />
present only briefly, the corresponding<br />
antibody response<br />
is likely to be persistent; iii)<br />
the half-life <strong>of</strong> antibodies is<br />
about 15 days which minimises<br />
daily fluctuations; iv) antibodies<br />
<strong>are</strong> highly stable comp<strong>are</strong>d<br />
to many other serum proteins<br />
making serum-handling protocols<br />
less stringent; v) the amplification<br />
cascade controlled by<br />
the humoral immune system<br />
causes a surplus <strong>of</strong> circulating<br />
antibodies after appearance <strong>of</strong><br />
the cognate (low-abundance)<br />
antigen. Circulating IgGs can<br />
be monitored in a bottomup<br />
ELISA setup, meaning<br />
that the reactive serum IgG is<br />
sandwiched between the antigen,<br />
which is immobilised<br />
in a microtitre plate, and the<br />
labelled anti-human IgG detection<br />
antibody. Antigen (micro)<br />
arrays allow the simultaneous,<br />
multiplexed measurement<br />
<strong>of</strong> serum antibodies against<br />
multiple antigens. In addition,<br />
fluid-phase assay systems<br />
based on antigens coupled to<br />
addressable beads have been<br />
developed [4,6,7]. The latter<br />
systems may be best suited<br />
<strong>for</strong> future implementation <strong>of</strong><br />
multiplexed antigen assays in<br />
clinical laboratories.
11<br />
– February/March 2011<br />
Colon tumour antigens<br />
Colon tumour antigens have<br />
been identified by different<br />
approaches, including blotting<br />
<strong>of</strong> colon tumour cell lines [8],<br />
phage display <strong>of</strong> a CRC cDNA<br />
library [9], and commercial<br />
protein microarrays [10]. In all<br />
these cases serum from CRC<br />
patients and controls is used<br />
to select those antigens that<br />
<strong>are</strong> specifically recognised by<br />
antibodies from the patient<br />
sera [4,6]. The sensitivity and<br />
specificity <strong>of</strong> single antigens <strong>for</strong><br />
detection was promising, but<br />
still below the required standards<br />
<strong>for</strong> diagnostic purposes. A<br />
higher accuracy was obtained<br />
by using a panel <strong>of</strong> antigens<br />
reaching a sensitivity and specificity<br />
both <strong>of</strong> 92%. The specificity<br />
<strong>of</strong> this test could even be<br />
further increased to 96% by the<br />
inclusion <strong>of</strong> carcino embryonic<br />
antigen (CEA) as marker in this<br />
panel [9]. In addition to protein<br />
antigens, an immune response<br />
to aberrant glycosylated mucins<br />
has also been implicated as a<br />
potential marker <strong>for</strong> CRC [11].<br />
Notably, however, the immune<br />
response against altered selfproteins<br />
from tumour cells is in<br />
general inferior to the response<br />
against antigens from an infectious<br />
agent. There<strong>for</strong>e, the close<br />
interaction <strong>of</strong> colonic (tumour)<br />
cells with intestinal bacteria<br />
may provide new opportunities<br />
<strong>for</strong> finding antigenic<br />
<strong>biomarkers</strong> <strong>for</strong> CRC.<br />
The colon: a hybrid<br />
super organ<br />
The colonic epithelium is in<br />
constant contact with an enormous<br />
number <strong>of</strong> bacteria (also<br />
known as microbiota or microbiome<br />
) that largely outnumber<br />
the epithelial cells. It is estimated<br />
that the human microbiota<br />
is composed <strong>of</strong> around 10 14<br />
bacterial cells, comprising >10 3<br />
species [12,13]. This dense bacterial<br />
population is essential <strong>for</strong><br />
digestion <strong>of</strong> food and control <strong>of</strong><br />
intestinal epithelial homeostasis.<br />
Thus, human and bacterial<br />
cells together <strong>for</strong>m a complex<br />
ecosystem that, as a whole,<br />
interactively per<strong>for</strong>ms various<br />
biological processes. In this way<br />
the colon can be regarded as a<br />
hybrid superorgan. It is important<br />
to know that inter-individual<br />
variations in microbiota<br />
composition <strong>are</strong> huge, whereas<br />
the intra-individual composition<br />
<strong>of</strong> intestinal microbiota<br />
is relatively stable throughout<br />
life [14,15]. Accumulating<br />
evidence also supports a<br />
relationship between certain<br />
mucosa-associated bacterial<br />
and intestinal diseases such as<br />
CRC. Two models <strong>for</strong> intestinal<br />
dysbiosis can be envisaged.<br />
First, disease-promoting bacteria<br />
that <strong>are</strong> part <strong>of</strong> the intrinsic<br />
microbiome <strong>of</strong> a certain individual<br />
induces epithelial damage.<br />
Second, a diseased state<br />
<strong>of</strong> the host epithelium, such as<br />
CRC, induces local microbiome<br />
dysbalance. Both models<br />
<strong>are</strong> discussed below.<br />
CRC-associated bacteria<br />
Several recent studies have<br />
provided mechanistic evidence<br />
<strong>for</strong> the involvement <strong>of</strong><br />
gut bacteria in the development<br />
<strong>of</strong> CRC, which includes<br />
the production <strong>of</strong> DNA damaging<br />
superoxide radicals,<br />
genotoxins or toxic metabolites<br />
and the induction <strong>of</strong> cell<br />
proliferation and/or pro-carcinogenic<br />
pathways. As intestinal<br />
microbiomes differ from<br />
individual to individual, the<br />
intrinsic intestinal microbiota<br />
<strong>of</strong> a specific person may contain<br />
an unfavourable number<br />
<strong>of</strong> pathogenic bacteria. In the<br />
long term, their activities may<br />
compromise the activities <strong>of</strong><br />
the health-promoting (commensal)<br />
bacterial population.<br />
For example, carcinogenic<br />
activities have been ascribed<br />
to certain Enterococcus faecalis,<br />
Escherichia coli and Bacteroides<br />
fragilis strains [16-<br />
20]. Monitoring the activity<br />
<strong>of</strong> this group <strong>of</strong> bacteria may<br />
thus be important <strong>for</strong> the risk<br />
assessment <strong>of</strong> CRC.<br />
On the other hand, the dramatic<br />
physiological and metabolic<br />
alterations that result from colon<br />
carcinogenesis itself disturbs the<br />
local intestinal microenvironment.<br />
This causes (local) shifts<br />
in microbiota composition as<br />
the altered tumour metabolites<br />
and intestinal physiology will<br />
recruit a bacterial population<br />
with a competitive advantage in<br />
this specific microenvironment.<br />
This is exemplified by infections<br />
<strong>of</strong> the opportunistic intestinal<br />
pathogen Streptococcus gallolyticus<br />
(aka Streptococcus bovis<br />
biotype I) that have been associated<br />
with CRC <strong>for</strong> many years<br />
[21,22]. This bacterial species<br />
can adhere to the collagens that<br />
become exposed to the intestinal<br />
lumen during the <strong>for</strong>mation<br />
<strong>of</strong> polyps [23]; pre-malignant<br />
sites appear to be a preferred<br />
niche <strong>for</strong> this bacterial species<br />
by which it can gain access to<br />
the human body. Importantly,<br />
most S. gallolyticus infections<br />
remain subclinical and thus may<br />
occur much more <strong>of</strong>ten than<br />
is currently realised. A similar<br />
mechanism may explain the<br />
association between Clostridium<br />
septicum and CRC [24]. The latter<br />
group <strong>of</strong> bacteria may play<br />
an important signalling role in<br />
CRC diagnostics.<br />
Microbiot<strong>are</strong>lated<br />
antigens<br />
In our laboratory, we investigated<br />
whether the occurrence<br />
<strong>of</strong> subclinical S. gallolyticus<br />
infections could be<br />
helpful in CRC diagnostics.<br />
Using an immunocapture mass<br />
www.cli-online.com & search 25431
– February/March 2011 12 Tumour markers<br />
spectrometry approach, we observed that<br />
associated antigen responses were diagnostic<br />
<strong>for</strong> both CRC and polyp patients<br />
[25,26]. The presence <strong>of</strong> serum IgG against<br />
ribosomal protein (Rp) L7/L12 was monitored<br />
in two independent sample collections<br />
using an ELISA-based approach.<br />
This demonstrated that anti-RpL7/<br />
L12 response was most pronounced in<br />
patients with early stage CRC and significantly<br />
different from that <strong>of</strong> healthy control<br />
subjects [27]. A drawback <strong>of</strong> the use<br />
<strong>of</strong> this antigen is its conservation in bacteria.<br />
Consequently, the cross reactivity <strong>of</strong><br />
this assay results in a large overlap in anti-<br />
RpL7/L12 titres between CRC cases and<br />
controls. The specificity <strong>for</strong> CRC was only<br />
57% at a sensitivity <strong>of</strong> 75%. Accordingly,<br />
current activities include the identification<br />
<strong>of</strong> alternative S. gallolyticus antigens that<br />
<strong>are</strong> more specific <strong>for</strong> this bacterial species.<br />
We anticipate that a broader approach will<br />
yield more accurate assays that may be<br />
applied on the individual level. This view<br />
is corroborated by a recent study showing<br />
that an ELISA-based assay using a mixture<br />
<strong>of</strong> surface proteins from S. gallolyticus as<br />
potential antigens yielded a similar sensitivity<br />
<strong>of</strong> 73%, but an improved specificity<br />
<strong>of</strong> 83% [28]. The identification <strong>of</strong> diagnostic<br />
antigens from other intestinal bacteria<br />
is also in progress. These include antigens<br />
from species such as S. gallolyticus, which<br />
take advantage <strong>of</strong> a pre-malignant lesion<br />
to invade the human body and thereby<br />
cause an antigen response, but antigens<br />
will also be sought from pathogenic bacteria<br />
that have been implicated in CRC<br />
initiation as discussed previously [Figure 1].<br />
FIigure 2. Hybrid antigen panels <strong>for</strong> the early<br />
diagnosis <strong>of</strong> CRC.<br />
Hybrid multimarker assays<br />
<strong>for</strong> CRC<br />
From a genetic perspective, CRC is a highly<br />
heterogeneous disease [29,30], which<br />
makes accurate diagnosis based on a single<br />
biomarker unlikely at the population level.<br />
On the contrary, multimarker assays <strong>are</strong><br />
likely to provide diagnostic plat<strong>for</strong>ms that<br />
can be used to screen populations <strong>for</strong> CRC<br />
and select high-risk individuals or individuals<br />
with early stage disease <strong>for</strong> follow up.<br />
As illustrated in Figure 1, certain mucosaassociated<br />
bacteria may be involved in<br />
CRC initiation. Invasiveness <strong>of</strong> these pathogens<br />
or exposure to their antigens may<br />
elicit an IgG response that is valuable <strong>for</strong><br />
CRC risk assessment in individuals. These<br />
individuals may not need a bowel examination<br />
immediately, but can be enrolled in a<br />
more strict monitoring programme. When<br />
an IgG response is detected against bacterial<br />
antigens that use polyps or tumours as<br />
a portal <strong>of</strong> infection, this may be an important<br />
sign <strong>of</strong> early stage disease, especially<br />
when IgGs against tumour antigens <strong>are</strong> also<br />
detected in the same subject [Figure 2]. It<br />
may be envisaged that immune responses<br />
against bacterial antigens decrease upon<br />
disease progression [27], whereas assays<br />
based purely on tumour antigens may<br />
leave early disease stages undetected.<br />
Thus a hybrid approach combines indirect<br />
bacterial markers that <strong>are</strong> associated<br />
with CRC risk and early stage disease with<br />
tumour markers that <strong>are</strong> diagnostic <strong>for</strong> the<br />
disease itself.<br />
Conclusions<br />
Hybrid antigen panels provide a promising<br />
new concept <strong>for</strong> CRC screening. However,<br />
much still needs to be learned about bacterial<br />
interference in CRC. It goes without<br />
saying that, when established, hybrid antigen<br />
panels would need a thorough clinical<br />
validation phase be<strong>for</strong>e decision algorithms<br />
based on these antigen panels can<br />
be developed.<br />
Acknowledgements<br />
The author would like to thank Annemarie Boleij,<br />
Rian Roel<strong>of</strong>s, Bas Dutilh, Wilbert Peters, Julian<br />
Marchesi and Ikuko Kato <strong>for</strong> inspiring discussions.<br />
The financial support from the Dutch Cancer Society<br />
(project KUN-2006-3591) and the Dutch Digestive<br />
Diseases Foundation (project WO10-53) <strong>for</strong><br />
our work on innovative CRC diagnostics is warmly<br />
acknowledged.<br />
References<br />
1. Jass JR, Morson BC. J Clin Pathol 1987; 40:<br />
1016-1023.<br />
2. Booth RA. Cancer Letters 2007; 249: 87-96.<br />
3. Simon J. N Engl J Med 1998; 338: 1151-1152.<br />
4. Tjalsma H. Exp Rev Proteomics 2010; 7: 879-895.<br />
5. Reuschenbach M, Kloor M, Morak M et al.<br />
Familial Cancer 2010; 9: 173-179.<br />
6. Tjalsma H, Schaeps RMJ, Swinkels DW. Proteomics<br />
Clin Appl 2008; 2: 167-180.<br />
7. Vignali DA. J Immunol Methods 2000; 243:<br />
243-255.<br />
8. He YJ, Mou ZR, Li WL et al. Int J <strong>of</strong> Colorecta Dis<br />
2009; 24: 1271-1279.<br />
9. Ran YL, Hu H, Zhou Z et al. Clin Cancer Res 2008;<br />
14: 2696-2700.<br />
10. Babel I, Barderas R, Diaz-Uriarte R et al. Mol Cell<br />
Proteomics 2009; 8: 2382-2395.<br />
11. Silk AW, Schoen RE, Potter DM et al. Mol Immunol<br />
2009; 47: 52-56.<br />
12. Dethlefsen L, Eckburg PB, Bik EM et al. Trends<br />
Ecol Evol 2006; 21: 517-523.<br />
13. Qin JJ, Li RQ, Raes J et al. Nature 2010; 464:<br />
59-U70.<br />
14. Green GL, Brost<strong>of</strong>f J, Hudspith B et al. J Appl<br />
Microbiol 2006; 100: 460-469.<br />
15. Costello EK, Lauber CL, Hamady M et al. Science<br />
2009; 326: 1694-1697.<br />
16. Toprak NU, Yagci A, Gulluoglu BM et al. Clin<br />
Microbiol Infect 2006; 12: 782-786.<br />
17. Wang XM, Allen TD, May RJ et al. Cancer Res<br />
2008; 68: 9909-9917.<br />
18. Wu SG, Rhee KJ, Albesiano E et al. Nature Medicine<br />
2009; 15: 1016-U1064.<br />
19. Cuevas-Ramos G, Petit CR, Marcq I et al. Proc<br />
Natl Acad Sci USA 2010; 107: 11537-11542.<br />
20. Lee SH, Hu LL, Gonzalez-Navajas J et al. Nature<br />
Medicine 2010; 16: 665-U665.<br />
21. Hausen HZ. Int J Cancer 2006; 119: XI-XII.<br />
22. Boleij A, Schaeps RMJ, Tjalsma H. J Clin Microbiol<br />
2009; 47: 516-516.<br />
23. Boleij A, Muytjens C, Bukhari S et al. J Infect Dis<br />
2011; in press.<br />
24. Wentling GK, Metzger PP, Dozois EJ et al. Dis<br />
Colon Rectum 2006; 49: 1223-1227.<br />
25. Tjalsma H, Scholler-Guinard M, Lasonder E et al.<br />
Int J Cancer 2006; 119: 2127-2135.<br />
26. Tjalsma H, Lasonder E, Scholler-Guinard M et al.<br />
Proteomics Clin Appl 2007; 1: 429-434.<br />
27. Boleij A, Roel<strong>of</strong>s R, Schaeps RM et al. Cancer<br />
2010;116: 4014-4022.<br />
28. Abdulamir AS, Hafidh RR, Mahdi LK et al. BMC<br />
Cancer 2009;<br />
29. Kaiser J. Science 2006; 313: 1370-1370.<br />
30. Sjoblom T, Jones S, Wood LD et al. Science 2006;<br />
314: 268-274.<br />
The author<br />
Dr Harold Tjalsma<br />
Department <strong>of</strong> Laboratory Medicine (830),<br />
Nijmegen Institute <strong>for</strong> Infection, Inflammation<br />
and Immunity (N4i) & Radboud University<br />
Centre <strong>for</strong> Oncology (RUCO) <strong>of</strong> the Radboud<br />
University Nijmegen Medical Centre.<br />
P.O. Box 9101, 6500 HB Nijmegen<br />
The Netherlands<br />
Tel. +31-24-3618947<br />
e-mail: h.tjalsma@labgk.umcn.nl
Which was the only serum free light chain assay available<br />
when the IMWG published guidelines <strong>for</strong> multiple myeloma<br />
and related disorders in 2009?<br />
A. Freelite B. Serumlite<br />
C.<br />
Hevylite<br />
D.<br />
Combylite<br />
The experts know the answer.<br />
In 2009 the International Myeloma Working Group published guidelines recommending<br />
the measurement <strong>of</strong> serum free light chain concentrations as an aid in the diagnosis,<br />
prognosis and monitoring <strong>of</strong> multiple myeloma patients. The advice was based upon<br />
results obtained in extensive clinical trials using the polyclonal Freelite TM assays. 1<br />
Freelite, launched in 2001, has become a proven, trusted and vital tool used by key<br />
opinion leaders around the globe <strong>for</strong> management <strong>of</strong> patients with B cell dyscrasias.<br />
Make sure you follow the experts.<br />
Proven and trusted<br />
serum free light<br />
chain assays<br />
- ask <strong>for</strong> it by name<br />
1. Dispenzieri A, et al. International Myeloma Working Group Guidelines. Leukemia 2009; 23:215-224<br />
Freelite TM is a trademark <strong>of</strong> The Binding Site Group Ltd, Birmingham, UK.<br />
www.cli-online.com & search 25504<br />
The Binding Site Group Ltd<br />
Tel: +44 (0)121 456 9500 • info@bindingsite.co.uk • www.bindingsite.com<br />
The Specialist Protein Company
– February/March 2011 14 Tumour markers<br />
Molecular <strong>for</strong>ms <strong>of</strong> prostate specific<br />
antigen (PSA) in serum: clinical and<br />
analytical implications<br />
Prostate specific Antigen (PSA) is widely used as a disease biomarker<br />
<strong>for</strong> diagnosis and monitoring <strong>of</strong> prostate <strong>cancer</strong> (PCa). Numerous<br />
different immunoassays <strong>are</strong> available <strong>for</strong> the measurement <strong>of</strong><br />
PSA and its sub<strong>for</strong>ms in serum. The assays can be referenced to<br />
different laboratory standards and <strong>are</strong> not interchangeable. Patients<br />
and physicians should be aw<strong>are</strong> <strong>of</strong> which assay was used, and<br />
longitudinal monitoring should be per<strong>for</strong>med with the same test.<br />
by Dr Katharina Braun, Dr David Ulmert and Dr Hans Lilja<br />
Prostate-specific antigen (PSA) is a kallikrein-related<br />
peptidase encoded by a five<br />
exon gene 7.1 kb (KLK3), one <strong>of</strong> fifteen<br />
genes clustered in a 280 kb locus on the long<br />
arm <strong>of</strong> chromosome 19 in the cytogenic<br />
region q13.3-4 [1]. KLK3 (encoding PSA)<br />
and KLK2 (encoding kallikrein-related<br />
peptidase 2 or hK2) sh<strong>are</strong> approximately<br />
80% amino acid sequence identity and the<br />
two proteins <strong>are</strong> produced and secreted at<br />
highly abundant levels by prostate epithelium<br />
although some expression can also<br />
be detected in certain other extra-prostatic<br />
tissues [2].<br />
PSA is synthesised as a 261-amino-acid<br />
(aa) pre-pro precursor that is processed to a<br />
non-catalytic zymogen through removal <strong>of</strong><br />
a ≈17-aa signal peptide upon transfer to the<br />
endoplasmic reticulum, whereas the short<br />
activation peptide must be released, e.g. by<br />
hK2, to convert the non-catalytic ≈244-aa<br />
zymogen to the mature 237-aa catalytic<br />
single-chain PSA [2].<br />
Originally called gamma-seminoprotein,<br />
a seminal fluid protein was identified in<br />
1966 and characterised in 1971 by Hara et<br />
al [3]. The authors anticipated that the protein<br />
would be a potential marker <strong>for</strong> seminal<br />
fluid applicable in the field <strong>of</strong> <strong>for</strong>ensic<br />
medicine. In 1979, PSA was purified from<br />
prostatic tissue, and was later found to be<br />
identical to gamma-seminoprotein [4]. Subsequently,<br />
several studies recognised PSA<br />
as a potential marker <strong>for</strong> PCa [5]. The first<br />
assay <strong>for</strong> PSA in serum was developed by<br />
Kuriyama et al [6] shortly after Papsidero<br />
and coworkers [5] identified PSA in blood.<br />
PSA is synthesised in normal prostate epithelium,<br />
benign prostate hyperplasia (BPH)<br />
and all stages <strong>of</strong> prostate adenocarcinoma.<br />
The concentration <strong>of</strong> PSA in seminal fluid<br />
is up to 10⁶ fold higher than in blood [7].<br />
The median concentration <strong>of</strong> tPSA in blood<br />
is ≈0.7 ng/mL in healthy men at early middle<br />
age [8], whereas in advanced <strong>cancer</strong> the<br />
amount <strong>of</strong> PSA in the blood can increase up<br />
to 10,000 fold [7].<br />
Although recent data from the large population-based<br />
randomised trials in Europe<br />
and the US have demonstrated that PSAbased<br />
prostate <strong>cancer</strong> screening can reduce<br />
mortality from prostate <strong>cancer</strong> by about half<br />
after fourteen years, these important benefits<br />
<strong>are</strong> tempered by considerable overdetection<br />
and consequential risks <strong>for</strong> overtreatment<br />
associated with current screening modalities<br />
[9]. Risk <strong>of</strong> prostate <strong>cancer</strong> diagnosis,<br />
metastasis and death from prostate <strong>cancer</strong><br />
<strong>are</strong> very strongly associated with concentration<br />
<strong>of</strong> PSA in blood [8]. This strong rationale<br />
explains the widespread use <strong>of</strong> PSA as a<br />
key biomarker to assess disease risk, monitor<br />
therapeutic intervention and disease<br />
recurrence and as a key component in<br />
various prognostic models.<br />
Molecular <strong>for</strong>ms <strong>of</strong> PSA in serum<br />
PSA added to blood in vitro exists in three<br />
<strong>for</strong>ms: one fraction will occur complexed with<br />
inactivating protease inhibitors, one portion<br />
as non-complexed non-catalytic PSA, and a<br />
third as active PSA entrapped by macroglobulins<br />
[10]. However, the “total PSA” (tPSA)<br />
detected in clinical samples comprises the<br />
sum <strong>of</strong> the concentration <strong>of</strong> both free PSA<br />
and PSA complexed to protease inhibitor<br />
ACT [11]. Data from the original discovery<br />
and characterisation <strong>of</strong> the proportion <strong>of</strong> free<br />
PSA versus PSA-ACT complexes suggested a<br />
mean free-to-total PSA ratio <strong>of</strong> 22% (range<br />
7-50%) in patient’s serum samples [11]. Based<br />
on PSA-measurements at early middle age<br />
in a large, highly representative populationbased<br />
cohort <strong>of</strong> men, the median proportion<br />
<strong>of</strong> free-to-total PSA in blood has later been<br />
shown to be ≈33% (IQR 28%; 38%) [12].<br />
Complexed PSA<br />
In the blood circulation, the majority <strong>of</strong> noncatalytic<br />
PSA is covalently complexed with<br />
the protease inihibitor α1-antichymotrypsin<br />
(ACT or SERPINA5). Active PSA can also<br />
be enveloped by α-macroglobulins such as<br />
α2-macroglobulin (A2M) and pregnancy<br />
zone protein (PZP) [10]. Unlike the interactions<br />
with ACT, the complex-<strong>for</strong>mation<br />
with A2M or PZP does not inactivate PSA<br />
although it blocks catalytic PSA from access<br />
to protein substrates [10]. It is noteworthy<br />
that such macromolecules mask epitopes recognised<br />
by commercially available assays and<br />
thus stay undetected by these methods [1,11].<br />
Since the original discovery in the early 1990s<br />
it has been c<strong>are</strong>fully documented that the proportion<br />
<strong>of</strong> PSA-ACT is higher in men with<br />
PCa comp<strong>are</strong>d to men with BPH [6,10], that<br />
the free-to-total PSA ratio is an independent<br />
predictor <strong>of</strong> prostate <strong>cancer</strong> risk [9], and that<br />
the free-to-total PSA ratio enhances discrimination<br />
<strong>of</strong> men with BPH from those with evidence<br />
<strong>of</strong> PCa beyond that <strong>of</strong> total PSA alone<br />
[13]. A systematic review and meta-analysis <strong>of</strong><br />
66 subsequent studies found that the free-tototal<br />
PSA ratio (“%fPSA”) enhanced the accuracy<br />
in predicting the diagnostic outcome <strong>of</strong><br />
a prostate biopsy comp<strong>are</strong>d to that based on<br />
tPSA alone [14].<br />
Free PSA and sub<strong>for</strong>ms<br />
The non-complexed, free PSA in blood<br />
is a mixture <strong>of</strong> different inactive <strong>for</strong>ms<br />
circulating unattached to any plasma<br />
proteins. These inactive <strong>for</strong>ms can be<br />
separated into two main fractions: single<br />
chain “intact” <strong>for</strong>ms with or without<br />
truncated remainders <strong>of</strong> the short activation<br />
peptide, and <strong>for</strong>ms that <strong>are</strong> inactive<br />
due to internal cleavages. The most
15<br />
– February/March 2011<br />
studied <strong>for</strong>ms <strong>of</strong> the latter subgroup <strong>are</strong><br />
PSA with internal cleavages at Lys145-<br />
Lys146 (“nicked PSA”) or cleavages at<br />
Lys182-Ser183 (“BPSA”) [15].<br />
While free PSA in men with BPH is correlated<br />
with a higher ratio <strong>of</strong> internally cleaved<br />
PSA, increased concentration <strong>of</strong> intact noncomplexed<br />
<strong>for</strong>ms and truncated precursor<br />
<strong>for</strong>ms <strong>of</strong> PSA <strong>are</strong> found in patients with<br />
presence <strong>of</strong> prostate <strong>cancer</strong> [16].<br />
Serum PSA measurement<br />
More than 80 antibodies against PSA have<br />
been very c<strong>are</strong>fully characterised based on<br />
their binding regions on the protein [17].<br />
Because <strong>of</strong> the high degree <strong>of</strong> amino acid<br />
sequence identity between PSA and hK2<br />
(80% identity), many monoclonal antibodies<br />
(MAbs) against PSA cross-react with hK2 –<br />
also with identical binding affinity to each <strong>of</strong><br />
these two highly similar proteins.<br />
Three distinct antigenic regions <strong>of</strong> PSA can<br />
be identified in reference to the ability to recognise<br />
free PSA, both free and complexed<br />
PSA, and the cross reactivity with hK2 [17].<br />
Non-linear antigenic domains that <strong>are</strong> in<br />
close proximity to amino acids 86-91 <strong>are</strong><br />
highly specific <strong>for</strong> free PSA. Epitopes specific<br />
<strong>for</strong> PSA without cross reactivity with hK2 <strong>are</strong><br />
located at or close to amino acids 158-163.<br />
The sh<strong>are</strong>d epitopes between PSA and hK2<br />
<strong>are</strong> located close to amino acids 3-11, which<br />
<strong>are</strong> close to the identical amino-terminal end<br />
<strong>of</strong> both proteins. Knowledge <strong>of</strong> antibody specificity<br />
is important <strong>for</strong> selecting appropriate<br />
antibody pairs when designing immunoassay<br />
[17]. Numerous commercial immunoassays<br />
<strong>are</strong> available <strong>for</strong> the measurement <strong>of</strong> PSA<br />
and its sub<strong>for</strong>ms in serum. Specific assays<br />
<strong>for</strong> fPSA as well as dual assays <strong>for</strong> fPSA and<br />
tPSA, PSA-ACT assays and hK2 assays have<br />
been developed [18 - 21]. Additionally assays<br />
detecting different proPSA <strong>for</strong>ms have been<br />
made available <strong>for</strong> use in research.<br />
There appears to be no access to any <strong>of</strong> the<br />
antigenic PSA epitopes subsequent to a stable<br />
complex that <strong>for</strong>med between PSA and<br />
α2 Macroglobulin (A2M), which makes<br />
measurement <strong>of</strong> PSA-A2M technically complicated<br />
and not clinically in<strong>for</strong>mative [22].<br />
Alternatively, denaturation with sodium<br />
dodecyl sulphate at high pH can be used to<br />
disrupt the PSA-A2M complex and release<br />
PSA from this complex, which then can be<br />
detected with a conventional ELISA [23].<br />
During the past two decades, multiple studies<br />
comp<strong>are</strong>d PSA <strong>value</strong>s measured by commercially<br />
available immunoassays with - at least<br />
in part - inconsistent and conflicting results.<br />
Graves et al comp<strong>are</strong>d the polyclonal assay<br />
from Yang laboratories with the Hybritech<br />
two site monoclonal assay in 1990 using<br />
samples from a group <strong>of</strong> 27 patients, and<br />
found a two-fold difference in PSA-levels<br />
between the two assays [24]. Semjonow et al<br />
reported a correction factor <strong>of</strong> 0.94 to 2.35<br />
when comparing Beckman Coulter Access<br />
and Hybritech Tandem E assays in 1996 [25].<br />
In contrast to these findings, Roehrborn et al,<br />
comparing three monoclonal based assays in<br />
a group <strong>of</strong> 86 patients (Hybritech Tandem E,<br />
Abbott ImX and Tosoh AIA 600) found no<br />
differences <strong>for</strong> total PSA [26]. Leewansangtong<br />
et al also reported a high correlation<br />
<strong>of</strong> PSA level ranges between the Hybritech<br />
Tandem E and Abbott AxSYM assay [27].<br />
Figure 1 illustrates one <strong>of</strong> the novel duallabel<br />
monoclonal antibody tests designed<br />
to selectively measure both fPSA as well as<br />
simultaneously enabling detection <strong>of</strong> total<br />
PSA with equimolar detection <strong>of</strong> free PSA<br />
and PSA-ACT complex [12].<br />
In 1994, the Second Stan<strong>for</strong>d Conference<br />
on International Standardisation <strong>of</strong> International<br />
Standards proposed the use <strong>of</strong> a standard<br />
produced by Stamey et al. This standard<br />
calibrator is composed <strong>of</strong> 90% PSA-ACT<br />
www.cli-online.com & search 25049
– February/March 2011 16 Tumour markers<br />
and 10% fPSA, similar to the distribution<br />
found in the circulation <strong>of</strong> PCa patients [28].<br />
This 90:10 PSA preparation was established<br />
as the World Health Organisation standard<br />
(WHO 96/670) [29]. PSA assays using the<br />
WHO 96/670 standard yield 20-25% lower<br />
PSA <strong>value</strong>s than those using the Hybritech<br />
standards [30].<br />
In 2004 Link et al comp<strong>are</strong>d the Beckman<br />
Coulter Access and Bayer Centaur system<br />
as well as the third generation DCP Immulite<br />
System, and found higher PSA <strong>value</strong>s<br />
measured with Access than Centaur and<br />
similar results with the Centaur and Immulite<br />
systems [31]. Blijenberg et al comp<strong>are</strong>d<br />
the Hybritech Tandem E, Beckman Coulter<br />
Access, DCP Immulite, Roche Diagnositcs<br />
Elecsys and Defia Prostatus systems and<br />
showed similar measurements <strong>for</strong> total<br />
PSA but not <strong>for</strong> fPSA [32].<br />
These findings were confirmed by two<br />
recent studies comparing equimolar assays<br />
calibrated to WHO standards. Kort et al<br />
comp<strong>are</strong>d tPSa, fPSa and cPSA in 70 samples<br />
in 6 different assays (Beckman Coulter<br />
Access, Abbott ARCHITECTS and Abbott<br />
AxSYM, Bayer Centaur, DPC Immulite<br />
2000, Roche Modular Analytics E170).<br />
Results showed variation in <strong>value</strong>s <strong>for</strong> tPSA<br />
from 0.5 to 1.0µg/L and <strong>for</strong> fPSA from 0.12<br />
to 0.40µg/L. Overall results showed less<br />
diversity <strong>for</strong> tPSA than fPSA, but tPSA<br />
assays were still not interchangeable [33].<br />
Stephan et al investigated the interchangeability<br />
<strong>of</strong> tPSA, fPSA and %fPSA between<br />
Beckman Coulter Access, DPC Immulite<br />
2000, Abbott AxSYM, Bayer Centaur and<br />
Roche Diagnositcs Elecsys assays and still<br />
found significant interassay variability.<br />
This may be due to the different epitope<br />
specificity <strong>of</strong> the antibodies used [34].<br />
Figure 1. Design <strong>of</strong> immunoassay <strong>for</strong> simultaneous<br />
measurement <strong>of</strong> free, uncomplexed <strong>for</strong>ms <strong>of</strong> PSA<br />
and total PSA. Monoclonal antibodies coated on<br />
plate as capture antibody <strong>for</strong> free and complexed<br />
<strong>for</strong>ms in equimolar fashion (Mab1). Monoclonal<br />
antibodies to detect PSA-ACT and free PSA (Mab2)<br />
and monoclonal antibodies accessible <strong>for</strong> fPSA<br />
epitope only (Mab3), both measureable<br />
with fluorescence (27).<br />
Conclusion<br />
Since the introduction <strong>of</strong> WHO 96/670<br />
Standards and development <strong>of</strong> tPSA-assays<br />
designed to detect free PSA and PSA-ACT<br />
on an equimolar basis, inter-assay variability<br />
has decreased – in particular regarding<br />
tPSA <strong>value</strong>s. Nevertheless results <strong>of</strong> commercially<br />
available tPSA assays <strong>are</strong> not yet<br />
interchangeable, not uni<strong>for</strong>mly standardised,<br />
and with no widely accepted conversion<br />
factor to correct the accuracy. Large<br />
discrepancies in fPSA <strong>value</strong>s may result in<br />
clinical misinterpretation as the decision to<br />
consider a prostate biopsy may be based on<br />
the ratio <strong>of</strong> fPSA to tPSA.<br />
Persisting discrepancies between assays<br />
result from a combination <strong>of</strong> the overall<br />
design, epitope specificity and affinity<br />
<strong>of</strong> capture and detector antibodies, use<br />
<strong>of</strong> monoclonal or polyclonal antibodies,<br />
cross-reactivity and non-specific interferences,<br />
as well as standardisation. Physicians<br />
should there<strong>for</strong>e be aw<strong>are</strong> <strong>of</strong> which assay<br />
and standards have been used and note<br />
whether the same test is also being used <strong>for</strong><br />
longitudinal monitoring <strong>of</strong> their patients.<br />
Acknowledgements<br />
Grant support: Swedish Cancer Society, Swedish<br />
Research Council (Medicine), The Tegger Foundation,<br />
Lund University Medical Faculty ALF grants,<br />
the National Cancer Institute [P50-CA92629], the<br />
Sidney Kimmel Center <strong>for</strong> Prostate and Urologic<br />
Cancers, David H. Koch through the Prostate<br />
Cancer Foundation, Fundación Federico SA, and<br />
German Association <strong>of</strong> Urology (DGU), Ferdinand<br />
Eisenberger research grant Competing interest<br />
declaration: Dr Hans Lilja holds patents <strong>for</strong> free<br />
PSA and hK2 assays.<br />
References<br />
1. Lilja H. J Clin Invest 1985;76:1899-1903<br />
2. Schedlich LJ, Bennetts BH, Morris BJ. DNA 1987;6:429-437<br />
3. Hara M, Koyanagi Y, Inoue T, Fukuyama T. Nihon Hoigaku<br />
Zasshi 1971;25:322-324<br />
4. Graves HC, Kam<strong>are</strong>i M, Stamey TA. J Urol 1990;<br />
144:1510-1515<br />
5. Papsidero LD, Wang MC, Valenzuela LA, Murphy GP, Chu<br />
TM. Cancer Res 1980;40:2428-2432<br />
6. Kuriyama M, Wang MC, Lee CI, et al. Cancer Res 1981;<br />
41:3874-3876<br />
7. Lundwall A, Clauss A, Olsson AY. Biol Chem 2006;<br />
387:243-249<br />
8. Lilja H, Cronin AM, Dahlin A, et al. Cancer 2010<br />
9. Craw<strong>for</strong>d ED, Grubb R, 3rd, Black A, et al. J Clin Oncol 2011;<br />
29:355-361<br />
10. Christensson A, Laurell CB, Lilja H. Eur J Biochem 1990;<br />
194:755-763<br />
11. Lilja H, Christensson A, Dahlen U, et al. PClin Chem 1991;<br />
37:1618-1625<br />
12. Lilja H, Ulmert D, Bjork T, et al. J Clin Oncol 2007;25:431-436<br />
13. Christensson A, Bjork T, Nilsson O, et al. J Urol 1993;<br />
150:100-105<br />
14. Roddam AW, Duffy MJ, Hamdy FC, et al. Eur Urol 2005;<br />
48:386-399; discussion 398-389<br />
15. Mikolajczyk SD, Millar LS, Wang TJ, et al. Urology 2000;<br />
55:41-45<br />
16. Nurmikko P, Pettersson K, Piironen T, Hugosson J, Lilja H.<br />
Clin Chem 2001 ;47:1415-1423<br />
17. Stenman UH, Paus E, Allard WJ, et al. Tumour Biol 1999;20<br />
Suppl 1:1-12<br />
28. Nurmikko P, Vaisanen V, Piironen T, et al. Clin Chem 2000;<br />
46:1610-1618<br />
18. Black MH, Grass CL, Leinonen J, Stenman UH, Diamandis<br />
EP. Clin Chem 1999; 45:347-354<br />
19. Zhu L, Leinonen J, Zhang WM, Finne P, Stenman UH. Clin<br />
Chem 2003; 49:97-103<br />
20. Bjork T, Piironen T, Pettersson K, et al. Urology 1996;<br />
48:882-888<br />
21. Piironen T, Lovgren J, Karp M, et al. Clin Chem 1996;<br />
42:1034-1041<br />
22. Lilja H, Haese A, Bjork T, et al. J Urol 1999;162:2029-2034;<br />
discussion 2034-2025<br />
23. Baumgart Y, Otto A, Schafer A, et al. Clin Chem 2005;<br />
51:84-92<br />
24. Graves HC, Wehner N, Stamey TA. J Urol 1990;<br />
144:1516-1522<br />
25. Semjonow A, Brandt B, Oberpenning F, Roth S, Hertle L.<br />
Prostate Suppl 1996; 7:3-16<br />
26. Roehrborn CG, Gregory A, McConnell JD, Sagalowsky AI,<br />
Wians FH, Jr. Urology 1996; 48:23-32<br />
27. Leewansangtong S, Goktas S, Lep<strong>of</strong>f R, Holthaus K, Craw<strong>for</strong>d<br />
ED. Urology 1998; 52:467-469<br />
28. Prestigiacomo AF, Chen Z, Stamey TA. Scand J Clin Lab<br />
Invest Suppl 1995; 221:57-59<br />
29. Rafferty B, Rigsby P, Rose M, Stamey T, Gaines Das R. Clin<br />
Chem 2000; 46:1310-1317<br />
30. Stamey TA. Urol Clin North Am 1997;24:269-273<br />
31.Link RE, Shariat SF, Nguyen CV, et al. J Urol 2004;171:<br />
2234-2238<br />
32. Blijenberg BG, Yurdakul G, Van Zelst BD, et al. BJU Int 2001;<br />
88:545-550<br />
33. Kort SAR, Martens F, Vanpoucke H, van Duijnhoven HL,<br />
Blankenstein MA. Clinical Chemistry 2006;52:1568-1574<br />
34. Stephan C, Klaas M, Muller C, et al. Clin Chem<br />
2006;52:59-64<br />
The authors<br />
Katharina Braun 1,5 , David Ulmert 1,3,4 and<br />
Hans Lilja 1,2,3<br />
Departments <strong>of</strong> 1 Surgery (Urology), 2 Clinical<br />
Laboratories, and Medicine, Memorial Sloan-<br />
Kettering Cancer Center, New York, USA<br />
Departments <strong>of</strong> 3 Laboratory Medicine, and<br />
4<br />
Urology, Lund University, Skåne University<br />
Hospital, Malmö, Sweden<br />
5<br />
Department <strong>of</strong> Urology, Marienhospital<br />
Herne, University Bochum, Herne, Germany<br />
Corresponding author:<br />
Hans Lilja, MD, PhD.<br />
Memorial Sloan-Kettering Cancer Center<br />
Department <strong>of</strong> Clinical Laboratories, Urology,<br />
1275 York Avenue, Box 213, New York, NY<br />
10065, USA<br />
e-mail: liljah@mskcc.org
Solutions<strong>for</strong> Life Science<br />
Your SANYO<br />
SANYO Biomedical<br />
freezers <strong>of</strong>fer<br />
outstanding reliability<br />
and per<strong>for</strong>mance<br />
-86°C ULT VIP Freezers<br />
Where SANYO took the<br />
initiative, the others<br />
followed<br />
-150°C Freezer<br />
MDF-C2156VAN<br />
The world’s largest<br />
capacity (231 litres)<br />
Isothermal Freezers<br />
No liquid Nitrogen<br />
contact<br />
As a storage environment,<br />
with excellent safety<br />
features, easy operability,<br />
and a host <strong>of</strong> other features,<br />
these freezers <strong>of</strong>fer<br />
unsurpassed reliability and<br />
functionality.<br />
SANYO’s VIP ULT freezers<br />
with patented vacuum<br />
insulation construction,<br />
microprocessor controls,<br />
high-per<strong>for</strong>mance<br />
refrigeration and dual<br />
cooling provide the best<br />
possible sample security.<br />
Equipped with SANYO’s<br />
new Cool Safe compressor<br />
and third generation VIP<br />
insulation. The excellent<br />
durability and per<strong>for</strong>mance<br />
enables long-term storage<br />
at temperatures far below<br />
the recrystallization point.<br />
With the Isothermal<br />
concept, samples can be<br />
stored safely in the -190°C<br />
range without the risk <strong>of</strong><br />
cross-contamination or<br />
direct contact <strong>of</strong> liquid<br />
Nitrogen when removing<br />
racks and samples from<br />
the freezer.<br />
SANYO E&E Europe BV<br />
Nijverheidsweg 120<br />
4879 AZ Etten Leur<br />
The Netherlands<br />
Tel: +31 (0)76 543 38 33<br />
Fax: +31 (0)76 541 37 32<br />
Email: export.eu.seee@sanyo.com<br />
http://eu.sanyo.com/biomedical<br />
www.cli-online.com & search 25367
– February/March 2011 18 Tumour markers<br />
Myeloma screening <strong>for</strong> the 21 st century<br />
The role <strong>of</strong> the serum free light chain assay* continues to evolve.<br />
Dr Jerry Katzmann, Laboratory Director Mayo Clinic, Rochester,<br />
USA addressed this topic from a laboratorian’s perspective at<br />
the recent 6 th International Symposium on Clinical Applications<br />
<strong>of</strong> Serum Free Light Chain Analysis. This thought-provoking<br />
presentation and what it means <strong>for</strong> the future is discussed.<br />
by Alison M. Levoguer and Richard G. Hughes<br />
Historical perspective:<br />
the oldest tumour marker<br />
Monoclonal Bence-Jones protein from myeloma<br />
patients, named after Dr Henry Bence<br />
Jones’ initial description, is the oldest tumour<br />
marker available. It is essential that both clinical<br />
chemists and clinical laboratory staff know<br />
how to recognise it. Such analysis is normally<br />
made by protein electrophoresis, which<br />
detects and quantifies an abnormal protein<br />
band (or M-spike), and immun<strong>of</strong>ixation electrophoresis,<br />
which identifies heavy and light<br />
chain types. Together these techniques provide<br />
diagnostic and monitoring in<strong>for</strong>mation<br />
but do not provide prognostic insights.<br />
Historically, in multiple myeloma (MM)<br />
the recommendation has always been to<br />
obtain a serum and urine sample from the<br />
patient, since the light chains produced by<br />
the tumour clone <strong>are</strong> excreted in the urine.<br />
The quantitative serum free light chain (FLC)<br />
assay has, since its availabilty in 2001, caused<br />
a phase shift in this idea. This can be elegantly<br />
demonstrated from data published in<br />
2001 [1] by plotting non – secretory multiple<br />
myeloma (NSMM) patients’ serum free light<br />
chain <strong>value</strong>s on a logarithmic kappa/ lambda<br />
FLC dot plot. Doing so shows this approach<br />
to be an effective tool <strong>for</strong> diagnosing NSMM<br />
from serum tests alone [Figure 1]. Second,<br />
because it is quantitative, this test allows<br />
monitoring <strong>of</strong> the patient response to treatment.<br />
Subsequent studies have provided<br />
further insights into the analogous diseases<br />
<strong>of</strong> light chain deposition and have revolutionised<br />
the diagnosis <strong>of</strong> AL amyloidosis [2].<br />
This is because such diseases <strong>are</strong> difficult to<br />
identify and quantitate by electrophoresis yet<br />
amenable to detection and quantification by<br />
serum free light chain assay. Since then, further<br />
studies have supported this initial work.<br />
Perhaps it is now time to reconsider the absolute<br />
need <strong>for</strong> undertaking urinalysis at initial<br />
diagnostic screening.<br />
<strong>Screening</strong> <strong>for</strong> plasma cell<br />
proliferative disorders (PCD)<br />
The current International Myeloma Working<br />
Group (IMWG) recommendation [3] <strong>for</strong><br />
myeloma screening is a panel combination<br />
<strong>of</strong> three serum tests; protein electrophoresis,<br />
immun<strong>of</strong>ixation electrophoresis and quantitative<br />
free light chain assay. There is little<br />
reason to per<strong>for</strong>m urine studies as part <strong>of</strong><br />
an initial diagnostic screening panel unless<br />
primary amyloidosis is suspected clinically.<br />
Once a plasma cell disorder (PCD) is diagnosed,<br />
urine studies should be carried out.<br />
This has an enormous impact on a clinical<br />
Figure 1. Serum FLC concentrations in patients with NSMM comp<strong>are</strong>d with normal individuals and<br />
patients with light chain multiple myeloma (LCMM). Reproduced from Serum Free Light Chain Analysis<br />
Sixth Edition, AR Bradwell 2010.<br />
laboratory. There is no need <strong>for</strong> two types<br />
<strong>of</strong> samples – pertinent since obtaining a 24<br />
hour urine collection is <strong>of</strong>ten difficult. A single<br />
serum sample allows the laboratory to<br />
carry out all IMWG screening panel tests.<br />
The sole reason <strong>for</strong> a urine sample request<br />
at screening is now <strong>for</strong> urine total protein<br />
assessment, its distribution and to quantitate<br />
any large M-spike if present. This small<br />
change in practice has a big potential impact.<br />
Dr Katzmann’s lab showed this in a study <strong>of</strong><br />
1,877 newly diagnosed PCD patients where<br />
all serum and urine tests were per<strong>for</strong>med [4].<br />
In per<strong>for</strong>ming all the tests that can be carried<br />
out in the clinical chemistry laboratory,<br />
namely serum protein electrophoresis (PEL),<br />
serum immun<strong>of</strong>ixation electrophoresis (IFE)<br />
and the serum free light chain assay as well as<br />
urine immun<strong>of</strong>ixation electrophoresis (urine<br />
IFE) nearly all, but not every patient can be<br />
detected: whilst powerful tests, interaction<br />
and dialogue with clinical colleagues <strong>are</strong><br />
still necessary to make a diagnosis in some<br />
cases. This is particularly true <strong>of</strong> light chain<br />
diseases (2% amyloid cases missed) and<br />
extramedullary <strong>for</strong>ms <strong>of</strong> myeloma.<br />
Retaining free light chain testing but omitting<br />
urine studies does miss diagnosing a<br />
few more patients, but not cases <strong>of</strong> myeloma,<br />
Waldenström’s macroglobulinaemia or<br />
smoldering myeloma (SMM). Some MGUS<br />
patients (by definition a pre-malignant disorder,<br />
predominantly laboratory defined)<br />
and 1% more amyloidosis cases <strong>are</strong> indeed<br />
missed. Overall, adding serum free light<br />
chain testing increases sensitivity with only<br />
a small concomitant decrease from omitting<br />
urine studies.<br />
In conclusion, none <strong>of</strong> these assays works<br />
successfully on its own. Assays should be<br />
used in combination to provide an effective<br />
screening panel. As we look to future laboratory<br />
and clinical practice, an effective PCD<br />
screening panel does not require urinalysis<br />
unless primary amyloidosis is suspected and<br />
may not require serum IFE. Dr Katzmann<br />
suggests that this may be reflected in the next<br />
iteration <strong>of</strong> the IMWG Guidelines.<br />
Prognosis – benign<br />
versus malignant<br />
monoclonal gammopathies<br />
Patient prognosis is another <strong>are</strong>a that<br />
impinges on laboratory practice. Since<br />
the free light chain assay has been found<br />
to be prognostic in every PCD studied<br />
so far, including the significant number<br />
* Freelite, Binding Site, UK
BD Viper System with XTR Technology<br />
Fast track to Molecular testing success<br />
Rising prevalence and a better understanding<br />
<strong>of</strong> underlying health<br />
risks <strong>are</strong> increasing the demand <strong>for</strong><br />
testing <strong>of</strong> Chlamydia trachomatis<br />
(CT) and Neisseria gonorrhoeae (GC),<br />
Herpes Simplex Virus 1 & 2 (HSV1 &<br />
HSV2)*, and Human Papillomavirus<br />
(HPV)* in targeted populations<br />
around the world.<br />
This demand comes at a time when<br />
laboratories <strong>are</strong> challenged by the<br />
pressure to contain healthc<strong>are</strong> costs,<br />
a shortage <strong>of</strong> trained personnel and<br />
expectations to deliver more results<br />
and higher quality results with fewer<br />
resources.<br />
Outpace your workload<br />
by streamlining your<br />
workflow<br />
The BD Viper System with XTR<br />
Technology meets these challenges<br />
with fully automated molecular<br />
testing that can put you on<br />
the fast track to molecular testing<br />
success.<br />
Fully automated sample processing<br />
• Complete automation: On board DNA extraction<br />
and real time amplification and detection<br />
• Walk-away convenience: Load and go capability<br />
allows technicians to get more work done<br />
• High throughput molecular testing: Continuous<br />
batching, 2 hours and 40 minutes <strong>for</strong> the first<br />
184 CT/GC results, 184 CT/GC results every<br />
1 hour 40 minutes following the first results<br />
Total system integrity<br />
• Results integrity: Excellent sensitivity and<br />
specificity proven in published clinical studies<br />
and independent pr<strong>of</strong>iciency surveys<br />
• System integrity: Unique “Reliability by<br />
Design” delivers maximum uptime<br />
• BD integrity: Around-the-clock customer service<br />
and support to ensure customer success<br />
• Minimum hands on time: Less than 20<br />
minutes hands on time per run, ready to<br />
use and unit dose based reagents<br />
* Products under evaluation, not available <strong>for</strong> sale or use.<br />
BD and BD Logo <strong>are</strong> trademarks <strong>of</strong> Becton, Dickinson and Company. ©2011 BD<br />
Becton Dickinson GmbH Tullastrasse 8-12, D-69126 Heidelberg. Germany. Sitz: Heidelberg. Geschäftsführer: Matthias Borst Amtsgericht Mannheim HRB 330 707.<br />
BD Diagnostics<br />
Tullastr. 8-12<br />
69126 Heidelberg<br />
Germany<br />
Tel. +49-6221 3050<br />
Fax +49 6221 305603<br />
www.bd.com<br />
www.cli-online.com & search 25508
– February/March 2011 20 Tumour markers<br />
<strong>of</strong> pre-malignant MGUS and SMM cases<br />
that <strong>are</strong> diagnosed each year, it is important<br />
to have a strategy <strong>for</strong> managing<br />
“benign monoclonal gammopathies” versus<br />
“malignant monoclonal gammopathies”.<br />
A study <strong>of</strong> 1,384 MGUS cases from<br />
a South Eastern Minnesota, USA cohort<br />
demonstrated that 1% <strong>of</strong> MGUS patients<br />
progressed to myeloma per year, the size<br />
<strong>of</strong> the M-spike and heavy chain isotype<br />
being prognostic <strong>for</strong> progression [5]. This<br />
was extended to include a third factor –<br />
an abnormal serum free light chain ratio<br />
and a risk stratification model was developed<br />
that identified “very low risk MGUS<br />
patients” using low serum monoclonal<br />
protein levels, IgG isotype and a normal<br />
serum free light chain ratio [6]. These<br />
MGUS patients’ disease progression rate<br />
was 0.1% per year. Whilst not synonymous<br />
with a “normal case” it is consistent<br />
with placement at the benign end <strong>of</strong><br />
the monoclonal gammopathy disease<br />
spectrum. Conversely, MGUS patients at<br />
very high risk <strong>are</strong> starting to be identified;<br />
the risk is not necessarily high enough at<br />
presentation to warrant immediate treatment,<br />
but these patients <strong>are</strong> most likely to<br />
exhibit the clinical symptoms and signs<br />
required (i.e. by CRAB criteria) <strong>for</strong> a<br />
diagnosis <strong>of</strong> myeloma in the future.<br />
11-12% <strong>of</strong> MGUS patients<br />
undetected by a simplified<br />
screening panel <strong>of</strong> serum PEL and<br />
FLC: should we be concerned?<br />
If MGUS patients’ lab tests <strong>are</strong> negative with<br />
serum protein electrophoresis and free light<br />
chain assay, with a small M-spike and a normal<br />
free light chain ratio, thus there is no, or<br />
just one adverse prognostic factor, they <strong>are</strong><br />
placed in a low risk group. There is a very<br />
low probability <strong>of</strong> progressing to disease and<br />
it may be preferable that laboratorians and<br />
clinicians do not identify them. This avoids<br />
placing a psychological burden on patients<br />
and an economic strain on the healthc<strong>are</strong><br />
system. More incumbent is to examine why<br />
recommendations <strong>for</strong> monitoring these individuals<br />
<strong>are</strong> what they <strong>are</strong>. Our patients’ lifelong<br />
interests <strong>are</strong> probably better served if<br />
Assay<br />
Coefficient <strong>of</strong><br />
Variability<br />
Figure 2. Serum FLC terminology: involved, uninvolved<br />
and difference in free light chain derivation.<br />
their clinical symptoms and signs <strong>of</strong> disease<br />
<strong>are</strong> monitored in the community by their<br />
primary healthc<strong>are</strong> physician in the first<br />
instance, as opposed to extensive lab-based<br />
monitoring under the hospital out-patient<br />
c<strong>are</strong> <strong>of</strong> a haematologist.<br />
Monitoring<br />
The free light chain immunoassay is recommended<br />
<strong>for</strong> monitoring <strong>of</strong> oligosecretory<br />
PCD (AL, NSMM, LCDD), that is, those<br />
patients who do not have a measurable<br />
serum or plasma M-spike and <strong>for</strong> documenting<br />
a response to therapy [6,7]. The recommendation<br />
<strong>for</strong> what a partial response (PR)<br />
is in these oligosecretory PCD patients has<br />
been set at a 50% reduction in the involved<br />
free light chain or dFLC [Figure 2].<br />
Dr Katzmann presented newly generated<br />
data from stable patients addressing the total<br />
coefficient <strong>of</strong> variation (CV) <strong>of</strong> some <strong>of</strong> these<br />
screening panel assays i.e., the biological and<br />
analytical variation combined. This patient<br />
cohort was not receiving therapy, had a stable<br />
diagnosis over time and blood was sampled<br />
every few months [Figure 3]. These data<br />
show that serum M-spike quantitation has a<br />
CV <strong>of</strong> 6.1% implying that a minimal change<br />
is approximately 12.2% in M-spike (i.e. 2<br />
standard deviations) with confidence in a<br />
partial reduction at 50%. Less change could<br />
be due to chance alone or evolution <strong>of</strong> disease<br />
over time. Immunoglobulin quantitation has<br />
a similar CV. The urine M-spike, in sharp<br />
contrast, has a CV that is much higher at<br />
29.1%, in accordance with a minimal change<br />
Analytic CV<br />
Biologic CV<br />
Serum M-spike [SPE] 6.1% 5% 3.5%<br />
Serum Ig [nephelometry] 9.9% 5% 8.5%<br />
Urine M-spike [SPE] 29.1% 6% 28.5%<br />
iFLC 26.0% 6% 25.3%<br />
rFLC 38.1%<br />
Figure 3. Coefficients <strong>of</strong> variability <strong>of</strong> monoclonal protein measurements in stable patients. Personal<br />
communication, Dr. Katzmann, February 2011. Reproduced with permission. iFLC = involved FLC,<br />
rFLC = free light chain ratio.<br />
in a urine M-spike, which itself necessitates at<br />
least a 50% change to define it correctly and<br />
more than a 90% reduction to consider it a<br />
partial response.<br />
A long held assumption has been that this<br />
very high variability was due to the quirks<br />
associated with 24 hour urine collection.<br />
However, when Katzmann examined the<br />
CV <strong>for</strong> the free light chain assays these data<br />
[Figure 3] showed a very similar CV to that<br />
<strong>of</strong> urine M-spike quantitation. So <strong>for</strong> both<br />
assays, despite low analytical CVs [Figure 3,<br />
column 3], some biological CV common to<br />
both [Figure 3, column 4] leads to a higher<br />
overall coefficient <strong>of</strong> variation. This biological<br />
variation is related to the light chains<br />
themselves in a way that is currently not fully<br />
understood but is most likely related to the<br />
short half lives <strong>of</strong> the free light chains. Table 3<br />
shows that biological variability <strong>of</strong> the serum<br />
free light chains, measured in this study at<br />
25.3% as well as last year [8] is similar to that<br />
<strong>for</strong> the urine M-spike at 28.5%. With this in<br />
mind a review <strong>of</strong> the IMWG guidelines is<br />
timely. From these data there is no reason to<br />
think that serum free light chain analysis is<br />
inferior to urinalysis, but criteria should be<br />
used <strong>for</strong> sFLC assay changes that <strong>are</strong> comparable<br />
to those currently used <strong>for</strong> urine assays.<br />
Perhaps it is time <strong>for</strong> a 90% reduction in FLC<br />
to be considered a partial response. In conclusion<br />
we should both honour the past contribution<br />
made by Henry Bence Jones but also<br />
address the need <strong>for</strong> assays to become more<br />
stringent and standardised internationally.<br />
References<br />
1. Drayson M et al. Blood 2001; 97: 2900-2902.<br />
2. Lachmann HJ et al. Br J Haematol 2003; 122: 78-84.<br />
3. Dispenzieri A et al. Leukemia 2009; 23: 215-224.<br />
4. Katzmann JA et al. Clin Chem 2009: 55:<br />
1517-1522.<br />
5. Kyle RA et al. N Engl J Med 2002; 346: 564-569.<br />
6. Rajkumar SV et al. Blood 2005; 106: 812-817.<br />
7. Gertz MA et al. Am J Hematol 2005; 79:<br />
319-328.<br />
8. Snyder M et al. Blood 2009; 114: 1803a.<br />
Editors comments: clarifications to the IMWG<br />
criteria <strong>for</strong> coding CR and VGPR in patients in<br />
whom the only measurable disease is by serum<br />
FLC levels were published during the writing <strong>of</strong><br />
this manuscript:<br />
S. Vincent Rajkumar, Blood. Prepublished online<br />
Feb 3 2011;doi:10.1182/blood-2010-10-299487.<br />
The authors<br />
Alison Levoguer, Scientific Affairs Manager<br />
Richard Hughes, Senior Research Scientist<br />
The Binding Site Group Limited,<br />
Birmingham, UK<br />
www.cli-online.com & search 25501
Trans<strong>for</strong>ming<br />
the Lab<br />
Innovative solutions enabling clinicians<br />
to put patients first.<br />
Government mandates to the healthc<strong>are</strong> industry have<br />
refocused strategies by setting expectations to “empower<br />
and liberate clinicians to innovate.” NHS Trusts utilising<br />
Sunquest ICE OpenNet can be confident <strong>of</strong> complying<br />
with government requirements and providing patients with<br />
the best possible c<strong>are</strong>.<br />
ICE OpenNet is an innovation that enables multiple Trusts<br />
to transmit comprehensive patient in<strong>for</strong>mation quickly<br />
and securely. ICE OpenNet also provides web-based<br />
communication systems that enable patients to be more<br />
involved in their own c<strong>are</strong>.<br />
With a 10-year track record <strong>of</strong> clinical success, Sunquest<br />
ICE is utilised worldwide by more than 300,000 healthc<strong>are</strong><br />
pr<strong>of</strong>essionals to improve patient safety and enhance their<br />
ability to provide patient-centric c<strong>are</strong>.<br />
<strong>for</strong> more in<strong>for</strong>mation about solutions from sunquest,<br />
call +44 (0) 845 519 4010 or visit www.sunquestinfo.com.<br />
Trans<strong>for</strong>ming T he Lab<br />
www.cli-online.com & search 25467
– February/March 2011 22 Tumour markers<br />
Role <strong>of</strong> PSA iso<strong>for</strong>ms in improving<br />
PSA specificity in asymptomatic men<br />
An overview <strong>of</strong> the European Randomised Study <strong>of</strong> <strong>Screening</strong> <strong>for</strong><br />
Prostate Cancer (ERSPC) side studies indicates that biomarker panels<br />
would enhance accuracy <strong>of</strong> PCa screening in asymptomatic men [1].<br />
by Dr Chris Bangma<br />
The diagnosis <strong>of</strong> prostate <strong>cancer</strong> (PCa)<br />
continues to challenge both clinicians<br />
and their laboratory colleagues. With<br />
the incidence <strong>of</strong> PCa rising progressively<br />
each year, it is now the most common<br />
<strong>for</strong>m <strong>of</strong> malignancy amongst men<br />
in Europe. [2]. Prostate-specific antigen<br />
(PSA) has been the main driver <strong>for</strong> early<br />
detection <strong>of</strong> prostate <strong>cancer</strong>. Increasingly,<br />
over the last decade, we have seen how<br />
aw<strong>are</strong>ness <strong>of</strong> the PSA test has generated a<br />
storm <strong>of</strong> diagnostic activity, particularly in<br />
countries like the US, even in men with few<br />
or no symptoms.<br />
This tumour marker has attracted extraordinary<br />
scientific attention regarding its<br />
biochemical characteristics, epidemiological<br />
and clinical <strong>value</strong>, alongside huge<br />
commercial interest and increasing debate,<br />
even in the lay press [3, 4]. The level <strong>of</strong><br />
PSA at initial screening is highly indicative<br />
<strong>of</strong> PCa being diagnosed later in life<br />
– however, approximately half <strong>of</strong> <strong>cancer</strong>s<br />
detected in this way <strong>are</strong> found to be indolent<br />
[5]. It has always been recognised that<br />
many prostate <strong>cancer</strong> patients died with,<br />
rather than because <strong>of</strong>, their disease, but<br />
it was not <strong>for</strong>eseen that the impact <strong>of</strong> PSA<br />
screening <strong>of</strong> asymptomatic men would<br />
result in such a large number <strong>of</strong> indolent<br />
(slow growing) <strong>cancer</strong>s being detected.<br />
The ERSPC believes that the benefits <strong>of</strong><br />
screening would be significantly increased<br />
by the introduction <strong>of</strong> new <strong>biomarkers</strong><br />
such as PSA iso<strong>for</strong>ms [Figure 1], and<br />
Complexed PSA<br />
Total PSA<br />
Other<br />
inactive<br />
PSA<br />
Truncated<br />
proPSA<br />
Free PSA<br />
Figure 1. SA and PSA Iso<strong>for</strong>ms – overview.<br />
Adapted by Chris Bangma from original table<br />
published in European Journal <strong>of</strong> Cancer, Oct<br />
2010 [1].<br />
BPSA<br />
the subsequent development <strong>of</strong> a panel <strong>of</strong><br />
screening tests. The additional analysis it<br />
carried out <strong>of</strong> candidate markers provides<br />
early encouragement. So far, the most<br />
promising results have been obtained from<br />
the analysis <strong>of</strong> free PSA, proPSA, nicked<br />
PSA and hK2 [6]. The availability <strong>of</strong> a<br />
panel <strong>of</strong> such markers could increase the<br />
specificity and sensitivity <strong>of</strong> screening <strong>for</strong><br />
prostate <strong>cancer</strong>, enabling new strategies to<br />
be developed <strong>for</strong> monitoring and asessing<br />
patient risk. This would reduce unnecessary<br />
biopsies, with surgical intervention<br />
only <strong>of</strong>fered to men at the highest risk.<br />
The first breakthrough in assessing the<br />
effectiveness <strong>of</strong> PSA testing on PCa mortality<br />
assessment came in March 2009 with the<br />
publication <strong>of</strong> the ERSPC study (involving<br />
an overall follow-up <strong>of</strong> up to 12 years) [7].<br />
It reported an initial reduction <strong>of</strong> at least<br />
20% in mortality, which rose to approximately<br />
30% when adjustment was made <strong>for</strong><br />
non-attendance <strong>of</strong> men enrolled in the<br />
study [8].<br />
Solving the dilemma <strong>of</strong><br />
overdiagnosis<br />
The likelihood <strong>of</strong> being diagnosed with prostate<br />
<strong>cancer</strong> in later life is highly dependent<br />
on the level <strong>of</strong> PSA at initial screening. PSA<br />
increases more quickly over time in men who<br />
get detectable <strong>cancer</strong>. However, the ERSPC<br />
study highlighted the serious limitations <strong>of</strong><br />
current PSA testing – that <strong>of</strong> overdiagnosis.<br />
In order to save one life, 1410 men would<br />
have to be tested and 48 men diagnosed with<br />
prostate <strong>cancer</strong>. To achieve this, an unacceptably<br />
high number <strong>of</strong> biopsies would<br />
subsequently be found to be negative.<br />
Current clinical practice uses a serum PSA<br />
<strong>value</strong> <strong>of</strong> more than 4 ng/mL to indicate<br />
abnormality; this is likely to lead to a prostatic<br />
biopsy. The case is less clear cut with<br />
men with a serum PSA between 2-4ng/mL.<br />
After undergoing a biopsy, 20 -30% <strong>of</strong> these<br />
men will be seen to have PCa, and <strong>of</strong> those,<br />
approximately one third <strong>of</strong> these <strong>cancer</strong>s<br />
<strong>are</strong> indolent and unlikely to cause death [9].<br />
Many patients have there<strong>for</strong>e undergone an<br />
unnecessary, invasive procedure– at a cost<br />
to both the men themselves and the health<br />
service involved. Based on the annual incidence,<br />
it is estimated that the annual number<br />
<strong>of</strong> unnecessary biopsies is around 750,000 in<br />
the US alone [10, 11].<br />
Throughout the duration <strong>of</strong> the study, the<br />
eight ERSPC countries involved used total<br />
PSA <strong>value</strong> as the sole indicator <strong>for</strong> biopsies.<br />
However, the study involved such a large<br />
sample (182,000 participants initially) that it<br />
was possible to carry out a number <strong>of</strong> additional<br />
country-specific studies specifically<br />
focusing on different candidate markers.<br />
Alongside evaluating changes in PSA concentrations<br />
over time (PSA velocity, PSA<br />
doubling), various PSA-iso<strong>for</strong>ms, kallikreins<br />
and molecular markers were assessed retrospectively<br />
in different ERSPC cohorts <strong>of</strong> men<br />
both with and without prostate <strong>cancer</strong>. The<br />
objective was to see what additional in<strong>for</strong>mation<br />
these candidate markers could add to<br />
the total PSA result hopefully enabling more<br />
selective PCa screening models to be developed<br />
<strong>for</strong> asymptomatic men.<br />
PSA is a kallikrein-like serine protease (also<br />
known as kallikrein-related peptidase 3),<br />
which is cleaved into smaller fragments as<br />
part <strong>of</strong> its biological pr<strong>of</strong>ile. Family members<br />
include kallikrein-related peptidase 2 (hK2),<br />
which is genetically and structurally very<br />
similar to PSA and also primarily localised to<br />
the epithelial cells <strong>of</strong> the prostate. hK2 rapidly<br />
converts the inactive precursor <strong>for</strong>m <strong>of</strong> PSA,<br />
proPSA, to active PSA and appears to be more<br />
strongly associated with prostate tumours<br />
than total PSA, being highly expressed in<br />
poorly differentiated <strong>cancer</strong> cells.<br />
Candidate markers —<br />
a brief glimpse at the possibilities<br />
From the side studies, the most promising<br />
potential <strong>biomarkers</strong> included % free PSA<br />
and free PSA <strong>for</strong>ms (intact/nicked PSA<br />
and proPSA) and hK2 [6]. ProPSA is found<br />
in normal prostatic epithelium together<br />
with truncated <strong>for</strong>ms. Mikolajczyk et al.<br />
identified a clinically important <strong>for</strong>m, (-2)<br />
proPSA, containing 239 amino acids. This<br />
<strong>for</strong>m is found in prostate <strong>cancer</strong> tissue as<br />
well as serum [12]. Indications <strong>are</strong> that the
23<br />
– February/March 2011<br />
various precursor <strong>for</strong>ms <strong>of</strong> PSA contribute<br />
unique predictive <strong>value</strong>s.<br />
The use <strong>of</strong> free PSA in addition to total<br />
PSA has been shown to reduce the number<br />
<strong>of</strong> sextant negative biopsies at a PSA cut<strong>of</strong>f<br />
level <strong>of</strong> 3 ng/mL by 30 % — at a cost <strong>of</strong><br />
missing 10 % <strong>of</strong> detectable <strong>cancer</strong>s (which<br />
were found microscopically to be predominately<br />
well differentiated) [13].<br />
The Swedish cohort demonstrated that<br />
the kallikrein markers would considerably<br />
improve the detection <strong>of</strong> pCa and the<br />
accuracy <strong>of</strong> predicting high-grade tumours<br />
(Gleason score ≥7 at biopsy). Using the panel<br />
<strong>of</strong> four kallikrein markers, at a biopsy-threshold<br />
<strong>of</strong> a 20% risk <strong>of</strong> prostate <strong>cancer</strong>, would<br />
have reduced the number <strong>of</strong> biopsies by 57%<br />
and missed only 31 out <strong>of</strong> 152 low-grade and<br />
3 out <strong>of</strong> 40 high-grade <strong>cancer</strong>s [14].<br />
Men with these high-grade tumours appe<strong>are</strong>d<br />
to have significantly greater p2PSA/%fPSA<br />
ratios then those with tumours that were less<br />
aggressive or indolent. Adding more support<br />
<strong>for</strong> a multi-kallikrein panel, in the first round<br />
<strong>of</strong> a population screening study the Rotterdam<br />
section <strong>of</strong> the ERSPC showed how<br />
the panel was found to predict PCa in men<br />
with an elevated PSA. This would reduce<br />
the number <strong>of</strong> biopsies by 413 per 1000<br />
men while missing only 60 (out <strong>of</strong> 216) low<br />
grade <strong>cancer</strong>s, and one out <strong>of</strong> 43 high-grade<br />
<strong>cancer</strong>s [6].<br />
Based on ERSPC retrospective analysis, a<br />
range <strong>of</strong> studies demonstrated that the implementation<br />
<strong>of</strong> %fPSA in population screening<br />
would have resulted in a considerable<br />
increase in specificity at the cost <strong>of</strong> a small<br />
loss <strong>of</strong> sensitivity. %fPSA was shown to be<br />
statistically significant in the PSA level range<br />
<strong>of</strong> 3 to 10ng/mL. In a study <strong>of</strong> almost 10,000<br />
Swedish patients, based on a total PSA ≥3ng/<br />
mL combined with %fPSA ≤18% the <strong>cancer</strong><br />
detection rate would have been 14% higher<br />
with a positive predictive <strong>value</strong> <strong>of</strong> 36% [15].<br />
In a study involving 1726 patients, using a<br />
%fPSA cut-<strong>of</strong>f <strong>of</strong> 16% or less as an indicator<br />
<strong>for</strong> biopsy would have reduced the number<br />
<strong>of</strong> false-positive results by 37%, at the cost <strong>of</strong><br />
missing 11% <strong>of</strong> the detectable <strong>cancer</strong>s [16].<br />
A variety <strong>of</strong> free to total PSA ratios were also<br />
analysed prospectively in order to assess their<br />
relative sensitivity and specificity as indicators<br />
<strong>for</strong> biopsy [Table 1]. When PSA level<br />
was below 3ng/mL, a low %fPSA (
– February/March 2011 24 Tumour markers<br />
[20]. PCA3 was also added to the panel,<br />
but at a later stage.<br />
Call <strong>for</strong> pan-European bioBank to<br />
sh<strong>are</strong> data and speed validation<br />
Better strategies <strong>are</strong> needed <strong>for</strong> clinicians and<br />
their supporting laboratory teams seeking<br />
safe ways to avoid invasive treatment in men<br />
likely to have indolent <strong>cancer</strong>s. If clinicians<br />
<strong>are</strong> to wait be<strong>for</strong>e sending certain patients<br />
with PSA levels < 10 ng/mL <strong>for</strong> biopsy, they<br />
must be sure that indolent tumours can be<br />
more accurately diagnosed, and that robust<br />
clinical tools <strong>are</strong> available to more precisely<br />
indicate the need <strong>for</strong> intervention. The lack<br />
<strong>of</strong> validation <strong>of</strong> novel genomic or proteomic<br />
markers in tissue, blood, or urine is one <strong>of</strong><br />
the major restrictions. There <strong>are</strong> many examples<br />
<strong>of</strong> candidate markers reported in the<br />
literature, which <strong>are</strong> validated in subsets <strong>of</strong><br />
ERSPC cohorts, but the potential contribution<br />
<strong>of</strong> each candidate marker can only be<br />
fully established by simultaneous assessment<br />
in a large population-based cohort with a<br />
follow up <strong>of</strong> five to 10 years. This is being<br />
delayed by the lack <strong>of</strong> adequate repositories,<br />
in particular <strong>for</strong> urine, as well as the labourintensive<br />
isolation <strong>of</strong> genomic material from<br />
<strong>cancer</strong> cells from prostatic biopsies.<br />
What is needed is a pan - European biorepository<br />
to allow <strong>for</strong> simultaneous retrospective<br />
assessment <strong>of</strong> markers in relation to final<br />
disease outcome. Ownership <strong>of</strong> the samples<br />
themselves would remain with the source,<br />
but by the establishment <strong>of</strong> a virtual computerised<br />
biobank, data, comparison and assessment<br />
could be more comprehensively sh<strong>are</strong>d<br />
and evaluated. What would be especially useful<br />
would be to hold and comp<strong>are</strong> in<strong>for</strong>mation<br />
on serial serum markers from patients<br />
who had needed little intervention, or in<br />
whom intervention had been avoided <strong>for</strong> several<br />
years e.g., in men in ‘watchful waiting’ or<br />
active surveillance programmes, or in those<br />
with benign prostatic hyperplasia (BPH).<br />
Reference<br />
Parameter <strong>for</strong><br />
Biopsy<br />
As the ERSPC data matures, more is becoming<br />
known about the fate <strong>of</strong> men with and<br />
without prostate <strong>cancer</strong>s. Because <strong>of</strong> the<br />
close follow-up involved, the ERSPC study<br />
can shed light on the predictive <strong>value</strong> <strong>of</strong><br />
clinical and laboratory markers over time.<br />
Future screening appears to rest on the<br />
development <strong>of</strong> a panel <strong>of</strong> markers, alongside<br />
equations and individual risk assessments<br />
[21]. This combined in<strong>for</strong>mation<br />
would enable diagnostic teams to determine<br />
both the risk <strong>of</strong> PCa and, if present, whether<br />
it would be aggressive or indolent. The role<br />
<strong>of</strong> PSA is likely to change. It could be incorporated<br />
into a more comprehensive, and<br />
more specific, combination <strong>of</strong> tests within<br />
a kallikrein panel, or used initially, but followed<br />
by a more personalised risk assessment<br />
invoving more specific markers.<br />
References<br />
1. Bangma CH et al. Eur J Cancer 2010; (46) 3109-3119.<br />
2. Quinn M et al. BJU Int. 2002; 90:162-73.<br />
3. De Angelis G et al. Rev Urol 2007; 9(3):113-23.<br />
4. Hernandez J et al. Cancer 2004; 101(5): 894-904.<br />
5. Draisma G et al. J Natl Cancer Inst 2003; 95(12): 868-78.<br />
6. Vickers AJ et al. Clin Cancer Res 2010; 16(12): 3232-9.<br />
7. Schröder FH et al. New Eng J <strong>of</strong> Med 2009; 360:<br />
1320-1328<br />
8. Roobol MJ et al. Eur Urol 2009; 56, Issue 4 584-591<br />
9. Roehl KA et al. J Urol 2002; 168: 922.<br />
10. Jemal A et al. Cancer J Clin 2009; 59(4): 225-49.<br />
11. Fad<strong>are</strong> O et al. Arch Pathol Lab Med 2004; 128(5):<br />
557-60.<br />
12. Mikolajczyk SD et al. Cancer Res 2001; 61(18):<br />
6958-63.<br />
13. Bangma CH et al. Urology 1995; 46 (6) 773-8.Bangma<br />
CH et al. Urology 1995; 46 (6):779-784.<br />
14. Vickers AJ et al. BMC Med 2008; 6:19.<br />
15. Becker C et al. J Urol 2003; 170(4 Pt 1):1169-74.<br />
16. Bangma CH et al. Urology 1995; 46(6):773-8.<br />
17. Finne P et al. Eur Urol 2008; 54(2): 362-70.<br />
18. Raaijmakers R et al. Eur Urol 2007; 52(5): 1358-64.<br />
19. Haese A et al. Prostate 2001; 49(2): 101-9.<br />
20. Roobol MJ et al. Urology 2004; 63(2): 309-13;<br />
discussion 313-5.<br />
PSA range<br />
Raaijmakers et al [22] Total PSA 2-3<br />
Finne et al [17] No biopsy < 3<br />
Recker et al [23] FT ratio 4<br />
Roobol et al [21]<br />
PSA-doubling time<br />
< 4 years, PSA<br />
velocities<br />
1-2<br />
Finding<br />
%fPSA predictive <strong>for</strong><br />
aggressiveness, NOT<br />
<strong>for</strong> positive biopsy<br />
%fPSA < 15 strong<br />
predictor <strong>of</strong> later Pca<br />
Low <strong>cancer</strong> specificity<br />
<strong>of</strong> FT ratio<br />
No benefit <strong>of</strong> early<br />
rescreen<br />
No independent<br />
predictor <strong>for</strong> <strong>cancer</strong><br />
Table 1. Results from ERSPC’s Prospective ERSPC Side Studies. Adapted by Chris Bangma from<br />
original table published in European Journal <strong>of</strong> Cancer, October 2010 [1].<br />
21. Roobol MJ et al. Eur Urol 2010: 57 (1): 79-85.<br />
22. Raaijmakers R et al. J Urol 2004;171(6 Pt 1):2245-9.<br />
23. Recker F et al. J Urol 2001;166(3):851-5.<br />
24. Rietbergen JB et al. J Urol 1998;160(6 Pt 1):2121-5.<br />
The author<br />
Chris Bangma<br />
Director <strong>of</strong> the ERSPC and<br />
chairman & head <strong>of</strong> the department <strong>of</strong><br />
urology Erasmus Medical Center,<br />
Rotterdam, The Netherlands<br />
www.cli-online.com & search 25517<br />
Beckman Coulter’s novel marker<br />
and index improve probability<br />
<strong>of</strong> detecting PCa<br />
In Europe, Beckman Coulter, Inc., has recently<br />
introduced a new prostate disease marker,<br />
p2PSA, and the Prostate Health Index (phi)<br />
<strong>for</strong> the non-invasive identification <strong>of</strong> patients<br />
who <strong>are</strong> most likely to have a negative prostate<br />
biopsy.*<br />
The new marker, named Access Hybritech<br />
p2PSA, measures the [-2]proPSA molecule,<br />
an iso<strong>for</strong>m <strong>of</strong> free PSA. Studies have demonstrated<br />
that when p2PSA measurements <strong>are</strong><br />
combined with Access Hybritech PSA and free<br />
PSA measurements, the resulting index demonstrates<br />
a significant improvement in clinical<br />
specificity <strong>for</strong> prostate <strong>cancer</strong> detection, relative<br />
to PSA and % fPSA alone, in the PSA range<br />
2–10 ng/mL in men >50 years and with nonsuspicious<br />
digital rectal exam (DRE) findings<br />
[1]. The extra dimension <strong>of</strong>fered by the Prostate<br />
Health Index (phi) means that the lab can<br />
provide the clinician with an automatic calculation<br />
from the index using the PSA, free PSA<br />
and p2PSA test results. The phi result gives the<br />
probability <strong>of</strong> prostate <strong>cancer</strong>. It does this by<br />
providing a significant increase in specificity<br />
over total, free PSA, or %fPSA while maintaining<br />
the accepted <strong>cancer</strong> detection rate.<br />
CLI reported in late 2009 on the <strong>for</strong>thcoming<br />
findings <strong>of</strong> the first prospective study<br />
looking at the effectiveness <strong>of</strong> p2PSA and phi<br />
and these have now been published in The<br />
Journal <strong>of</strong> Urology. They have confirmed that<br />
the Beckman Coulter phi score demonstrates<br />
significantly higher clinical specificity <strong>for</strong><br />
prostate <strong>cancer</strong> detection relative to PSA and<br />
%fPSA alone in men in the PSA range 2-10<br />
ng/mL (using the Hybritech calibration <strong>of</strong><br />
PSA). Clinical interpretive criteria have been<br />
developed <strong>for</strong> men in this entire range [2].<br />
* Relates to Europe only<br />
1. Mikolajczyk SD, Marker KM, Millar LS et al. Cancer<br />
Res 2001; 61: 695<br />
2. Le BV, Griffin CR, Loeb S, Carvalha IGF, Kan D,<br />
Baumann NA, Catalona WJ. J Urol .2010; 183 Issue<br />
4 1355-1359
News in brief<br />
25<br />
– February/March 2011<br />
Simple test <strong>for</strong> aggressive<br />
lung adenocarcinoma<br />
in never-smokers<br />
An inexpensive immunohistochemistry<br />
test can effectively<br />
identify a sub-group <strong>of</strong> neversmoking<br />
lung <strong>cancer</strong> patients<br />
whose tumours express a molecule<br />
associated with increased<br />
risk <strong>of</strong> disease progression<br />
or recurrence. Researchers at<br />
the Mayo Clinic, Rochester,<br />
USA, found that 8% - 12% <strong>of</strong><br />
patients with lung adenocarcinoma<br />
who have never smoked<br />
carry tumours that express<br />
anaplastic lymphoma kinase<br />
(ALK). This subset <strong>of</strong> patients<br />
is at more than twice the risk <strong>of</strong><br />
experiencing disease progression<br />
or recurrence within five<br />
years <strong>of</strong> initial diagnosis comp<strong>are</strong>d<br />
to never-smokers whose<br />
lung adenocarcinoma tumours<br />
<strong>are</strong> ALK-negative. The ability<br />
to test <strong>for</strong> ALK status in these<br />
patients might help in selecting<br />
the most appropriate therapies.<br />
http://tinyurl.com/6c8c5nz<br />
tumours had mutations in<br />
the epidermal growth factor<br />
receptor (EGFR) gene. All were<br />
being treated with the drug<br />
erlotinib, which acts on the<br />
EGFR molecule. The researchers<br />
set out to find genes that<br />
predicted which patients<br />
would have a lasting benefit,<br />
and which would not. To do<br />
this, they used NanoString, an<br />
integrated digital technology<br />
with high levels <strong>of</strong> precision<br />
and sensitivity that detects<br />
AD-CLSI_AD-LabMedica.qxd 25/02/2011 10:29 Pagina 1<br />
expression levels <strong>of</strong> hundreds<br />
<strong>of</strong> genes in a single reaction.<br />
They examined the expression<br />
levels <strong>of</strong> 48 different genes in<br />
43 patients with EGFR-mutant<br />
non-small cell lung <strong>cancer</strong><br />
who were being treated with<br />
erlotinib, and found that AEG<br />
(astrocye elevated gene 1, also<br />
known as metadherin) was<br />
the strongest predictor <strong>of</strong> progression-free<br />
survival in these<br />
patients. Progression-free survival<br />
was 27 months <strong>for</strong> those<br />
with low AEG-1 expression,<br />
comp<strong>are</strong>d to 12 months <strong>for</strong><br />
those with high expression.<br />
AEG-1 is a <strong>cancer</strong>-associated<br />
gene with multiple functions<br />
that contribute to several<br />
hallmarks <strong>of</strong> <strong>cancer</strong> including<br />
drug-resistance. For those<br />
patients in the high-risk group,<br />
clinical oncologists can be prep<strong>are</strong>d<br />
<strong>for</strong> early progression<br />
and an appropriate alternative<br />
management strategy.<br />
http://tinyurl.com/5sxy5ev<br />
Oncogene AEG-1<br />
strongly predicts<br />
response to erlotinib<br />
treatment in<br />
EGFR-mutant<br />
lung <strong>cancer</strong><br />
21 st International Congress <strong>of</strong><br />
Clinical Chemistry and Laboratory Medicine<br />
19 th IFCC - EFCC European Congress <strong>of</strong><br />
Clinical Chemistry and Laboratory Medicine<br />
8 th Annual Meeting <strong>of</strong> the German Society <strong>of</strong><br />
Clinical Chemistry and Laboratory Medicine<br />
Researchers in the Spanish<br />
Lung Cancer Group (SLCG),<br />
in cooperation with Pangaea<br />
Biotech, in the USP Dexeus<br />
University Institute, Barcelona,<br />
Spain have identified a<br />
gene whose expression level<br />
strongly predicts how well certain<br />
lung <strong>cancer</strong> patients will<br />
respond to treatment with the<br />
drug erlotinib. The researchers<br />
studied 55 patients with nonsmall<br />
cell lung <strong>cancer</strong>, whose<br />
Berlin, Germany<br />
ICC Berlin - Internationales Congress Centrum<br />
15 - 19 May 2011<br />
MARK YOUR CALENDAR<br />
30 March 2011<br />
Deadline <strong>for</strong> reduced fee registration<br />
www.berlin2011.org
– February/March 2011 26 Molecular diagnostics<br />
Genetic <strong>biomarkers</strong> in colorectal <strong>cancer</strong><br />
Colorectal <strong>cancer</strong> is at the leading edge <strong>of</strong> the emerging era <strong>of</strong><br />
personalised oncology. Mutational analysis <strong>of</strong> the KRAS and BRAF<br />
oncogenes on tumour tissue is already in widespread clinical use<br />
to guide anti-epidermal growth factor receptor (EGFR) therapy, and<br />
additional promising molecular <strong>biomarkers</strong> <strong>are</strong> being evaluated.<br />
In this review, we detail both established and emerging genetic<br />
<strong>biomarkers</strong> <strong>of</strong> colorectal <strong>cancer</strong> that in<strong>for</strong>m on prognosis and predict<br />
treatment responses, and highlight pre-analytic and analytic factors<br />
that impact on the accuracy <strong>of</strong> genetic testing in solid tumour tissue.<br />
by Dr Carlos J Su<strong>are</strong>z, Dr Eric Q. Konnick and Dr Colin Pritchard<br />
the current standard <strong>of</strong> c<strong>are</strong> <strong>for</strong> CRC, and<br />
the topoisomerase-I inhibitor irinotecan.<br />
Most studies suggest that 5-FU <strong>of</strong>fers little<br />
benefit to patients with MSI CRC; however,<br />
lack <strong>of</strong> complete agreement in the literature<br />
has limited the use <strong>of</strong> MSI testing to guide<br />
5-FU therapy [3]. Several studies with irinotecan<br />
have demonstrated increased survival<br />
in patients with MSI-associated CRC<br />
[10, 11], but the data is limited. There<strong>for</strong>e,<br />
MSI testing in CRC is currently primarily<br />
used as a screening assay <strong>for</strong> Lynch syndrome,<br />
and much less frequently to guide<br />
prognosis or treatment [Table 1].<br />
Colorectal <strong>cancer</strong> (CRC) is the third most<br />
common <strong>cancer</strong> and the fourth most<br />
common cause <strong>of</strong> <strong>cancer</strong> deaths worldwide,<br />
with 1.2 million cases and 609,000<br />
deaths reported in 2008 [1]. Advances in<br />
our understanding <strong>of</strong> the pathogenesis<br />
and evolution <strong>of</strong> CRC have demonstrated<br />
that molecular features that <strong>are</strong> not easily<br />
inferred from traditional morphology can<br />
predict both prognosis and response to<br />
treatment. To better characterise the molecular<br />
variants <strong>of</strong> colon <strong>cancer</strong>, <strong>biomarkers</strong><br />
have been developed that assess the status<br />
<strong>of</strong> cellular pathways known to be associated<br />
with CRC prognosis and treatment<br />
response. Although many <strong>biomarkers</strong> have<br />
been investigated and proposed, the best<br />
validated and most clinically accepted<br />
<strong>biomarkers</strong> to date <strong>are</strong> those associated<br />
with microsatellite instability (MSI)/mismatch<br />
repair (MMR) system and the Epidermal<br />
Growth Factor Receptor (EGFR)<br />
signalling pathway. Here, we focus on established<br />
prognostic and predictive <strong>biomarkers</strong><br />
related to the EGFR signalling pathway<br />
and MSI/MMR system, with a brief discussion<br />
<strong>of</strong> several promising new <strong>biomarkers</strong><br />
[summarised in Table 1]. We conclude with<br />
Colorectal <strong>cancer</strong>: genetic <strong>biomarkers</strong> can in<strong>for</strong>m<br />
on prognosis and predict treatment responses.<br />
a discussion <strong>of</strong> laboratory considerations<br />
that influence biomarker detection and<br />
interpretation <strong>of</strong> results.<br />
Microsatellite instability (MSI) and<br />
the Mismatch Repair System<br />
Microsatellites <strong>are</strong> short segments <strong>of</strong> repetitive<br />
DNA that <strong>are</strong> prone to errors during<br />
DNA replication [2]. To correct these errors<br />
and prevent deleterious mutations, all species<br />
have a well-conserved DNA mismatchrepair<br />
(MMR) system, which comprises a<br />
group <strong>of</strong> proteins including MLH1, MSH2,<br />
MSH3, MSH6, and PMS2 in humans [3].<br />
Deficiencies in the DNA mismatch-repair<br />
system cause cumulative mutations in<br />
microsatellite sequences, leading to what is<br />
referred as microsatellite instability (MSI).<br />
Approximately 15% <strong>of</strong> all colorectal <strong>cancer</strong>s<br />
present with MSI [4, 5], and within<br />
those cases about 3% <strong>are</strong> associated with<br />
Lynch syndrome [5, 6], and ~12% <strong>are</strong> due<br />
to sporadically acquired deficiencies in the<br />
MMR system [7, 8]. In Lynch syndrome,<br />
also known as hereditary non-polyposis<br />
colorectal <strong>cancer</strong> (HNPCC), the functional<br />
alterations in the MMR system <strong>are</strong><br />
secondary to germline mutation in the<br />
MMR genes commonly affecting MLH1,<br />
MSH2 and MSH6. In contrast, the majority<br />
<strong>of</strong> sporadic MSI tumours <strong>are</strong> due to hypermethylation<br />
<strong>of</strong> the MLH1 promoter, resulting<br />
in gene silencing [9].<br />
Both germline and sporadic CRC tumours<br />
with MSI <strong>are</strong> less prone to invasion, metastasis,<br />
and lymph nodes spread, and have a<br />
better prognosis than their microsatellite<br />
stable (MSS) counterpart [8]. In addition,<br />
some studies have shown an association<br />
between MSI and response to adjuvant<br />
chemotherapy with 5-fluorouricil (5-FU),<br />
The EGF signalling pathway<br />
The discovery <strong>of</strong> EGFR expression in<br />
malignant cells, and its potential role in<br />
pathogenesis <strong>of</strong> malignancy, led to the<br />
development <strong>of</strong> monoclonal antibodies<br />
that could be used as targeted anti-<strong>cancer</strong><br />
therapy. It was quickly noted that not all<br />
CRC patients treated with the new anti-<br />
EGFR medications showed a demonstrable<br />
response, prompting a deeper investigation<br />
into the signalling pathways <strong>of</strong> EGFR.<br />
This lead to the realisation that mutations<br />
in CRC downstream <strong>of</strong> EFGR in the pathway<br />
allow <strong>for</strong> autonomous activation <strong>of</strong> the<br />
pathway, and subsequent activation <strong>of</strong> the<br />
mitogen activated kinase (MAPK) pathway,<br />
leading to signals which promote cell<br />
survival and growth.<br />
KRAS<br />
KRAS is a key downstream mediator <strong>of</strong><br />
EGFR signalling that is mutated in ~40% <strong>of</strong><br />
CRC. Activating mutations in KRAS codon<br />
12 and 13 <strong>are</strong> observed early in tumourigenesis,<br />
<strong>are</strong> conserved through <strong>cancer</strong><br />
progression, and <strong>are</strong> mutually exclusive <strong>of</strong><br />
BRAF mutations [12]. Mutations in KRAS<br />
codon 12 or 13 predict resistance to anti-<br />
EFGR therapy (cetuximab and panitumumab)<br />
[13-16], however, even patients<br />
with wild-type KRAS do not consistently<br />
respond to anti-EGFR therapy (~20-50%)<br />
[17]. Testing <strong>of</strong> neoplastic tissue is now the<br />
standard <strong>of</strong> c<strong>are</strong> <strong>for</strong> CRC patients who <strong>are</strong><br />
being considered <strong>for</strong> anti-EGFR therapy<br />
because <strong>of</strong> the near complete lack <strong>of</strong> drug<br />
response when KRAS is mutated.<br />
BRAF<br />
BRAF is a protein kinase downstream <strong>of</strong><br />
KRAS in the EFGR signalling pathway that<br />
is mutated in 10-15% <strong>of</strong> CRC. BRAF mutations<br />
occur about 10-times more frequently<br />
in MSI tumours (~50%) comp<strong>are</strong>d to MSS
27<br />
– February/March 2011<br />
CRC (~5%), and <strong>are</strong> mutually<br />
exclusive <strong>of</strong> KRAS mutations<br />
[12]. The majority <strong>of</strong> mutations<br />
<strong>are</strong> a single base pair substitution<br />
leading to a V600E change<br />
in the amino acid sequence.<br />
Patients with BRAF mutations<br />
have an app<strong>are</strong>nt decreased<br />
overall survival comp<strong>are</strong>d<br />
to patients with wild-type<br />
BRAF when treated with anti-<br />
EFGR therapy [18]. CRC with<br />
mutated BRAF do not appear<br />
to respond to monoclonal<br />
antibody treatment, although<br />
larger studies <strong>are</strong> needed to<br />
confirm the results observed to<br />
date [19]. BRAF inhibitors <strong>are</strong><br />
in various stages <strong>of</strong> development,<br />
and some <strong>are</strong> currently<br />
under evaluation in clinical trials,<br />
suggesting the possibility<br />
that BRAF mutational analysis<br />
may be used in the future to<br />
guide BRAF inhibitor therapy<br />
in CRC.<br />
Possible future<br />
<strong>biomarkers</strong><br />
PI3K/PTEN<br />
The phosphatidylinositol<br />
3-kinase (PI3K) pathway is<br />
thought to be involved in modulating<br />
EFGR signalling and is<br />
mutated in up to 40% <strong>of</strong> CRC.<br />
Mutations in the PI3K pathway<br />
<strong>are</strong> not mutually exclusive<br />
<strong>of</strong> KRAS or BRAF mutations.<br />
Deregulated signalling in this<br />
pathway has been linked to<br />
either an activating mutation<br />
in the PIK3CA p110 subunit or<br />
inactivation <strong>of</strong> the PTEN phosphatase.<br />
Studies have suggested<br />
that alterations in the PI3K/<br />
PTEN pathway lead to resistance<br />
to anti-EFGR treatment,<br />
although the association is not<br />
as definitive as observed in<br />
KRAS or BRAF [20, 21]. PI3K<br />
may also be a target <strong>for</strong> drug<br />
development, however, the<br />
utility in CRC may be impacted<br />
by the coexistence <strong>of</strong> PI3K and<br />
KRAS mutations [22].<br />
Loss <strong>of</strong> 18q<br />
The loss <strong>of</strong> the long arm <strong>of</strong> chromosome<br />
18 (18q) is observed<br />
in ~70% <strong>of</strong> CRC, and is associated<br />
with a worse prognosis,<br />
however results have not been<br />
consistent to date [23]. Several<br />
genes thought to be involved in<br />
predisposing to CRC, including<br />
trans<strong>for</strong>ming growth-factor<br />
beta (TGFβ) pathway mediators<br />
such as SMAD4 <strong>are</strong> located<br />
in this region. There <strong>are</strong> ongoing<br />
clinical trials evaluating the<br />
predictive utility <strong>of</strong> 18q status.<br />
Topoisomerase I<br />
Increased protein expression<br />
<strong>of</strong> topoisomerase, based on<br />
IHC, has been correlated with<br />
an increased response to the<br />
topoisomerase inhibitor irinotecan,<br />
and a decrease in IHC<br />
signal correlated with a lack <strong>of</strong><br />
additional benefit [24]. This<br />
is not surprising, given that<br />
irinotecan is a topoisomerase<br />
I inhibitor, but replication<br />
<strong>of</strong> these results is warranted<br />
be<strong>for</strong>e routine use <strong>of</strong> topoisomerase<br />
level determination<br />
to direct therapy decisions.<br />
Laboratory<br />
considerations<br />
Diagnosis <strong>of</strong> MSI and<br />
differentiation <strong>of</strong> sporadic<br />
CRC from Lynch<br />
Syndrome/HNPCC<br />
MSI can be suspected clinicopathologically<br />
in colon<br />
adenocarcinomas that <strong>are</strong><br />
right-sided, with focal mucinous<br />
differentiation, high histologic<br />
grade, absence <strong>of</strong> “dirty<br />
necrosis”, prominent tumourinfiltrating<br />
lymphocytes, and a<br />
Crohn’s-like host response [25].<br />
However, confirmation <strong>of</strong> the<br />
genetic alterations associated<br />
with MSI is necessary to make<br />
the diagnosis.<br />
Genetic diagnosis <strong>of</strong> MSI is<br />
primarily based on PCR amplification<br />
<strong>of</strong> specific microsatellite<br />
loci with fluorescent primers,<br />
and subsequent fragment<br />
analysis by capillary electrophoresis<br />
[26] . The length <strong>of</strong><br />
target microsatellite loci in<br />
tumour and normal cells from<br />
the same patient <strong>are</strong> comp<strong>are</strong>d,<br />
and if differences <strong>are</strong> identified<br />
in more than 30% <strong>of</strong> the loci<br />
analysed, a diagnosis <strong>of</strong> MSI is<br />
given (also referred to as MSIhigh,<br />
or MSI-H). When the differences<br />
only involve 10-29% or<br />
less than 10% <strong>of</strong> the loci, these<br />
findings <strong>are</strong> diagnosed as MSIlow<br />
and MSS, respectively. For<br />
both prognostic and predictive<br />
purposes, MSI-low and MSS <strong>are</strong><br />
usually considered equivalent.<br />
In 1997, an international consensus<br />
meeting [27] established<br />
a reference panel <strong>of</strong> 5 microsatellite<br />
loci (2 mononucleotide<br />
loci, BAT25 and BAT26, and<br />
3 dinucleotide loci, D5S346,<br />
D2S123 and D17S250) with<br />
high sensitivity and specificity<br />
<strong>for</strong> MSI, known as the Bethesda<br />
panel, and also established the<br />
a<strong>for</strong>ementioned cut-<strong>of</strong>f point<br />
to interpret results. Since then,<br />
other panels containing alternative<br />
loci, particularly mononucleotide<br />
loci that seem to<br />
be more specific <strong>for</strong> MSI than<br />
dinucleotide loci, have been<br />
developed. Currently, many<br />
molecular laboratories use<br />
panels <strong>of</strong> five mononucleotide<br />
loci including BAT25, BAT26,<br />
NR21, NR24 and MONO21.<br />
An alternative and complementary<br />
strategy <strong>for</strong> the diagnosis <strong>of</strong><br />
MSI is immunohistochemistry<br />
(IHC) analysis <strong>of</strong> MMR proteins.<br />
Antibodies against<br />
MLH1, MSH2, MSH6 and<br />
PMS2 <strong>are</strong> used to identify the<br />
loss <strong>of</strong> expression <strong>of</strong> any <strong>of</strong><br />
these MMR proteins. The per<strong>for</strong>mance<br />
<strong>of</strong> the IHC analysis<br />
has been estimated to be very<br />
similar to the MSI analysis with<br />
approximately >93% sensitivity<br />
and 100% specificity, although<br />
interobserver variability may<br />
be greater with IHC comp<strong>are</strong>d<br />
to MSI testing [28].<br />
Once the diagnosis <strong>of</strong> MSI<br />
has been established, it is<br />
critical to determine whether<br />
the MMR deficiency is due<br />
to Lynch syndrome or sporadically<br />
acquired MSI <strong>for</strong><br />
genetic counselling purposes.<br />
BRAF mutational analysis can<br />
help with this determination<br />
because ~50% <strong>of</strong> sporadic MSI<br />
tumours have BRAF mutations,<br />
whereas hereditary<br />
MSI tumours almost never<br />
have mutations in BRAF [12].<br />
However, a definite diagnosis<br />
<strong>of</strong> Lynch syndrome requires<br />
BioVendor’s Range <strong>of</strong> Cancer Biomarkers<br />
Cancer <strong>of</strong> Lung, Prostate, Ovary, Bone, Breast, Colon, Myeloma…<br />
ELISA kits to quantify<br />
Dickkopf-Related Protein 1 (Dkk1)<br />
GDF-15/MIC-1<br />
Free Light Chain κ and λ (FLC)<br />
sHER-2<br />
Midkine<br />
p53<br />
Prostate Secretory Protein 94 (PSP94)<br />
• serum, plasma, urine, cerebrospinal fluid<br />
• superior assay validation<br />
• simple, robust, user-friendly<br />
• excellent technical support<br />
Secretagogin<br />
TRAIL<br />
Trefoil Factor 1 (TFF1)<br />
Trefoil Factor 2 (TFF2)<br />
Trefoil Factor 3 (TFF3)<br />
Zinc-α-2-Glycoprotein (ZA2G)<br />
BioVendor – Laboratorni Medicina a.s., Karásek 1/1767, 621 33 Brno, Czech Republic<br />
Phone: +420 549 124 185, Fax: +420 549 211 460, E-mail: info@biovendor.com<br />
www.biovendor.com<br />
www.cli-online.com & search 25443
– February/March 2011 28 Molecular diagnostics<br />
germline sequencing and insertion/deletion<br />
analysis <strong>of</strong> the MMR genes. If the<br />
tumour has been previously analysed by<br />
immunohistochemistry, targeted germline<br />
sequencing and insertion/deletion<br />
analysis <strong>of</strong> the gene corresponding to the<br />
missing MMR protein can be per<strong>for</strong>med.<br />
Pre-analytic and analytic<br />
considerations <strong>of</strong> molecular<br />
diagnostic methods<br />
Genetic testing <strong>of</strong> solid tissue specimens<br />
presents a unique challenge <strong>for</strong> the clinical<br />
laboratory. Samples vary widely in tissue<br />
quantity (e.g. fine needle biopsy vs. resection<br />
specimen), quality (e.g. fresh frozen<br />
vs. <strong>for</strong>malin-fixed <strong>for</strong> 72 hours), and heterogeneity<br />
<strong>of</strong> tumour and non-tumour<br />
tissue. Due to these factors, highly robust<br />
and sensitive methods that can detect a<br />
clinically significant variant present in a<br />
low proportion <strong>of</strong> the sample <strong>are</strong> needed.<br />
Traditional Sanger sequencing has a sensitivity<br />
<strong>of</strong> only ~15-20% to detect minor<br />
allele populations within a mixture,<br />
which can result in false negative results<br />
<strong>for</strong> KRAS testing [29]. Pyrosequencing<br />
and melting curve analysis generally have<br />
better sensitivity, at ~1-10% [29]. Newer<br />
methods that increase sensitivity further<br />
to ~0.1-1% include co-amplification at<br />
lower denaturation temperature (COLD)-<br />
PCR, and peptide nucleic acid (PNA)<br />
clamping [30, 31]. Such sensitive methods<br />
have been described in the literature <strong>for</strong><br />
KRAS [30-32] and BRAF [32] mutation<br />
detection in CRC, and have been shown<br />
to improve diagnostic accuracy. Additional<br />
techniques which could allow ultrasensitive<br />
detection <strong>of</strong> somatic mutations<br />
include next-generation sequencing [33]<br />
and limiting-dilution-PCR [34]. Importantly,<br />
with the increased ability to detect<br />
minor mutant populations within the<br />
sample, it will be necessary to determine<br />
the clinically relevant threshold in addition<br />
to the absolute analytical threshold.<br />
Conclusions and<br />
recommendations<br />
Marked improvements in our understanding<br />
<strong>of</strong> CRC biology over the last few years<br />
have led to the discovery <strong>of</strong> several genetic<br />
<strong>biomarkers</strong> that guide treatment and<br />
establish prognosis <strong>of</strong> patients with CRC.<br />
Although many <strong>biomarkers</strong> have been<br />
studied, currently only KRAS, BRAF, and<br />
MSI <strong>are</strong> sufficiently validated to support<br />
routine clinical use. Cases in which MSI is<br />
suspected based on clinicopathologic data<br />
should be tested. If MSI is demonstrated,<br />
the distinction between Lynch syndrome<br />
and sporadic CRC is fundamental to determine<br />
the necessity <strong>of</strong> genetic counselling<br />
and close oncologic surveillance. Sporadic<br />
CRC cases should be evaluated <strong>for</strong> KRAS<br />
and possibly BRAF if anti-EGFR therapy is<br />
an option. In the future, testing the PI3K<br />
pathway genes PIK3CA and PTEN may<br />
help define the population which is most<br />
likely to benefit from the expensive anti-<br />
EGFR treatment. The per<strong>for</strong>mance <strong>of</strong> the<br />
molecular methods used <strong>for</strong> the above<br />
determinations needs to be considered<br />
and clearly communicated so that patients<br />
receive the most accurate and meaningful<br />
in<strong>for</strong>mation, and do not over-interpret the<br />
laboratory data.<br />
As the era <strong>of</strong> molecular oncology and<br />
personalised medicine unfolds, many<br />
changes in the way <strong>cancer</strong> is currently<br />
diagnosed and treated <strong>are</strong> expected to<br />
occur. Laboratory directors and staff alike<br />
have the responsibility <strong>of</strong> keeping up with<br />
the pace <strong>of</strong> change to continue <strong>of</strong>fering<br />
the best diagnostic testing to clinicians<br />
and patients.<br />
References<br />
1. Karsa LV et al. Best Pract Res Clin Gastroenterol<br />
2010; 24(4): 381-396.<br />
2. Boland CR et al. Gastroenterology 2010;<br />
138(6):2073-2087.e2073.<br />
3. Vilar E et al. Nat Rev Clin Oncol 2010; 7(3):153-162.<br />
Biomarker Freq. Detection Method Current Uses Possible Future Uses<br />
KRAS codon 12/13<br />
mutations<br />
40% DNA mutation testing Anti-EGFR resistance Prognosis<br />
BRAF V600E mutation 10% DNA mutation testing<br />
Microsatellite<br />
instability (MSI)<br />
15% PCR/sizing<br />
Anti-EGFR<br />
resistance,Lynch/<br />
HNPCC diagnosis<br />
Lynch/HNPCC<br />
diagnosis<br />
PIK3CA mutations 20% DNA mutation testing None<br />
BRAF inhibitor sensitivity<br />
Prognosis,5-FU<br />
resistance,Irinotecan<br />
sensitivity<br />
Anti-EGFR resistance,PI3K<br />
inhibitor sensitivity<br />
PTEN loss 30% IHC None Anti-EGFR resistance<br />
18q loss 50% FISH, cytogenetics None Prognosis<br />
Topoisomerase 1 low 50% IHC None Irinotecan sensitivity<br />
Freq.: Frequency in colorectal <strong>cancer</strong>; 5-FU: 5-fluorouracil; IHC: Immunohistochemistry; FISH:<br />
Fluorescent in situ hybridization<br />
Table 1. Genetic Biomarkers in colorectal <strong>cancer</strong>.<br />
4. Aaltonen LA et al. N Engl J Med 1998; 338(21):<br />
1481-1487.<br />
5. Hampel H et al. N Engl J Med 2005;<br />
352(18):1851-1860.<br />
6. Hampel H et al. J Clin Oncol 2008; 26(35):5783-5788.<br />
7. Ward R et al. Gut 2001; 48(6):821-829.<br />
8. Popat S et al. J Clin Oncol 2005; 23(3):609-618.<br />
9. Kane MF et al. Cancer Res 1997; 57(5):808-811.<br />
10. Fallik D et al. Cancer Res 2003; 63(18):5738-5744.<br />
11. Bertagnolli MM et al. J Clin Oncol 2009; 27(11):<br />
1814-1821.<br />
12. Rajagopalan H et al. Nature 2002; 418(6901):934.<br />
13. Bokemeyer C et al. J Clin Oncol 2009;<br />
27(5):663-671.<br />
14. Benvenuti S et al. Cancer Res 2007;<br />
67(6):2643-2648.<br />
15. Van Cutsem E et al. J Clin Oncol 2007; 25(13):<br />
1658-1664.<br />
16. Amado RG et al. J Clin Oncol 2008;<br />
26(10):1626-1634.<br />
17. Normanno N et al. Nat Rev Clin Oncol 2009; 6(9):<br />
519-527.<br />
18. Roth AD et al. J Clin Oncol 2010; 28(3):466-474.<br />
19. Di Nicolantonio F et al. J Clin Oncol 2008; 26(35):<br />
5705-5712.<br />
20. Jhawer M et al. Cancer Res 2008; 68(6):1953-1961.<br />
21. Sartore-Bianchi A et al. Cancer Res 2009; 69(5):<br />
1851-1857.<br />
22. Janku F et al. Mol Cancer Ther 2011.<br />
23. Popat S et al. Eur J Cancer 2005; 41(14):2060-2070.<br />
24. Braun MS et al. J Clin Oncol 2008; 26(16):2690-2698.<br />
25. Greenson JK et al. Am J Surg Pathol 2003; 27(5):<br />
563-570.<br />
26. Laghi L et al. Oncogene 2008; 27(49):6313-6321.<br />
27. Boland CR et al. Cancer Res 1998; 58(22):5248-5257.<br />
28. Shia J. J Mol Diagn 2008; 10(4):293-300.<br />
29. Tsiatis AC et al. J Mol Diagn 2010; 12(4):425-432.<br />
30. Milbury CA et al. Clin Chem 2009;<br />
55(12):2130-2143.<br />
31. Pritchard CC et al. BMC Clin Pathol England 2010;<br />
10: 6.<br />
32. Mancini I et al. J Mol Diagn 2010; 12(5):705-711.<br />
33. Mardis ER et al. Hum Mol Genet 2009; 18(R2):<br />
R163-168.<br />
34. Pohl G et al. Expert Rev Mol Diagn 2004; 4(1):41-47<br />
The authors<br />
Carlos J Su<strong>are</strong>z, Eric Q. Konnick and Colin<br />
Pritchard<br />
Department <strong>of</strong> Laboratory Medicine<br />
University <strong>of</strong> Washington<br />
Seattle, WA 98195, USA<br />
The authors contributed equally to this work.<br />
Corresponding author:<br />
Colin C. Pritchard MD, PhD<br />
University <strong>of</strong> Washington<br />
Department <strong>of</strong> Laboratory Medicine<br />
Molecular Diagnostics Laboratory, Room<br />
NW-275<br />
Seattle, WA 98195-7110, USA<br />
Tel. +1 206 598 6131<br />
Fax +1 206 598 6189<br />
e-mail: cpritch@uw.edu.
Microbiology<br />
29<br />
– February/March 2011<br />
Laboratory diagnosis <strong>of</strong> syphilis:<br />
indirect detection methods<br />
Due to diverse clinical manifestations which <strong>are</strong> sh<strong>are</strong>d with other<br />
treponemal and non-treponemal diseases, it is important to diagnose<br />
syphilis with the aid <strong>of</strong> appropriate and reliable laboratory tests.<br />
by Dr Meghna Patel<br />
Syphilis is a sexually transmitted disease<br />
caused by the spirochete, Treponema pallidum<br />
[1, 2]. It is a chronic disease with many<br />
very serious complications, especially during<br />
pregnancy, affecting the cardio-vascular<br />
and nervous systems in particular. It can also<br />
facilitate the transmission <strong>of</strong> HIV [2, 3]. During<br />
the course <strong>of</strong> the disease there <strong>are</strong> diverse<br />
clinical manifestations, which <strong>are</strong> indistinguishable<br />
from those <strong>of</strong> many other diseases<br />
[1, 4]. In recent years the incidence <strong>of</strong> syphilis<br />
has greatly increased in the United States and<br />
in Germany [1, 5]. Syphilis is easy to cure in<br />
the early stage, but can become disabling in<br />
the later stages and can ultimately be fatal [1].<br />
The disease progresses through four stages:<br />
the primary, secondary, latent and tertiary<br />
stages. The stage <strong>of</strong> the disease at which the<br />
patient presents has implications <strong>for</strong> diagnosis<br />
and treatment [6].<br />
There <strong>are</strong> several laboratory tests, which can be<br />
categorised into direct and indirect detection <strong>of</strong><br />
T. pallidum, to diagnose syphilis at the various<br />
stages <strong>of</strong> the disease. This article will focus on<br />
indirect detection methods; with direct methods<br />
there <strong>are</strong> difficulties in cultivation and<br />
maintenance <strong>of</strong> T. pallidum in the laboratory,<br />
and in samples from patients with the latent<br />
and late stages <strong>of</strong> the disease, there is a paucity<br />
<strong>of</strong> spirochetes <strong>for</strong> direct observation. However<br />
a good number <strong>of</strong> indirect detection methods<br />
have been developed and <strong>are</strong> routinely used to<br />
diagnose syphilis. Broadly these <strong>are</strong> classified<br />
as non treponemal and treponemal tests.<br />
Non treponemal tests<br />
These tests <strong>are</strong> <strong>of</strong>ten referred to as non specific,<br />
reagin or cardiolipin tests, as they use<br />
standardised antigen containing cardiolipin,<br />
cholesterol and lecithin to detect the presence<br />
<strong>of</strong> IgG and IgM antibodies to lipoidal material<br />
released from host cells [4]. US CDCapproved<br />
standard tests include the Venereal<br />
Diseases Research Laboratory (VDRL) slide<br />
test, the Rapid Plasma Reagin (RPR) card<br />
test, the Unheated Serum Reagin (USR) test<br />
and the Toluidine Red Unheated Serum Test<br />
(TRUST) [6]. Serum is preferred over plasma<br />
<strong>for</strong> both treponemal and non treponemal<br />
tests, however plasma can also be used <strong>for</strong> the<br />
RPR test and the TRUST. The VDRL and USR<br />
tests <strong>are</strong> micr<strong>of</strong>locculation tests that <strong>are</strong> read<br />
using a microscope. Even though the VDRL<br />
is the only test directly applicable <strong>for</strong> CSF testing,<br />
its utility is limited because the antigenic<br />
suspension is unstable and must be freshly<br />
prep<strong>are</strong>d every day <strong>for</strong> reliable results, and<br />
the serum sample must be heat-inactivated.<br />
However, the USR uses a very stable antigenic<br />
suspension and an unheated serum sample,<br />
which facilitates use. Being macroscopic flocculation<br />
tests, a microscope is not required to<br />
per<strong>for</strong>m the RPR and TRUST. The RPR uses a<br />
stabilised VDRL antigen containing charcoal<br />
particles to facilitate reading <strong>of</strong> the test. In the<br />
TRUST, charcoal is replaced by toluidine red<br />
dye that gives pink coloured floccules with<br />
positive samples. These tests can be used as<br />
both qualitative and semi-quantitative assays<br />
to determine the titre <strong>of</strong> the sample. Non<br />
treponemal tests <strong>are</strong> <strong>of</strong> great <strong>value</strong> <strong>for</strong> monitoring<br />
the course <strong>of</strong> the disease during and<br />
after treatment, and <strong>for</strong> diagnosis <strong>of</strong> reinfection<br />
and relapse.<br />
In spite <strong>of</strong> these advantages, non treponemal<br />
tests cannot be used alone <strong>for</strong> syphilis diagnosis<br />
as they have limited sensitivity, especially<br />
in primary and late latent syphilis patients,<br />
and the prozone phenomenon in secondary<br />
syphilis can result in false negatives. False positives<br />
can also occur due to cross reactivity in<br />
patients with hepatitis, chicken pox, infectious<br />
mononucleosis, measles, malaria and connective<br />
tissue disease, as well as in pregnancy [4].<br />
Span Diagnostic’s non treponemal tests RPR<br />
and TRUST provide stable, aqueous ready to<br />
use reagents with standardised immunoreactivity.<br />
They <strong>of</strong>fer simple, rapid and inexpensive<br />
test <strong>for</strong> syphilis and <strong>are</strong> even suitable <strong>for</strong> epidemiological<br />
and field studies. The company<br />
has further improved its non treponemal tests<br />
with the use <strong>of</strong> synthetic VDRL antigen, manufactured<br />
by US-FDA approved technology,<br />
licensed from the CDC. Synthetic VDRL antigen<br />
<strong>of</strong>fers better stability comp<strong>are</strong>d to natural<br />
VDRL antigen.<br />
Treponemal tests<br />
These <strong>are</strong> sometimes referred to as specific<br />
tests because they use T. pallidum or its components<br />
as antigen/s. Treponemal tests <strong>are</strong><br />
mainly used <strong>for</strong> confirming the results <strong>of</strong><br />
non treponemal tests that have low specificity.<br />
They <strong>are</strong> also important <strong>for</strong> detecting<br />
very early, congenital or late cases <strong>of</strong> syphilis<br />
when non treponemal tests <strong>are</strong> negative.<br />
However the usefulness <strong>of</strong> treponemal tests<br />
is limited by their cost and complexity, as<br />
well as by persistent positive results even in<br />
patients who have been successfully treated.<br />
In treponemal tests, anti-treponemal antibodies<br />
<strong>are</strong> detected by techniques such as<br />
agglutination, Enzyme Immuno Assay (EIA),<br />
immun<strong>of</strong>luorescence, immunoblotting and<br />
immunochromatogrphy.<br />
Indirect Agglutination tests<br />
The Treponema Pallidum HaemAgglutination<br />
(TPHA) and Treponema Pallidum Particle<br />
Agglutination (TPPA) tests <strong>are</strong> examples<br />
<strong>of</strong> indirect agglutination tests. In the TPHA<br />
classically sheep RBCs <strong>are</strong> coated with sonicated<br />
T. pallidum preparations. In positive<br />
samples these <strong>are</strong> agglutinated by the anti<br />
treponemal antibodies present. The TPHA<br />
is a highly sensitive test in all stages <strong>of</strong> the<br />
disease except in early primary syphilis. It is<br />
also reasonably specific but there <strong>are</strong> some<br />
false positives, from the use <strong>of</strong> sheep RBCs,<br />
in patients suffering from infectious mononucleosis,<br />
leprosy, collagen disease and other<br />
miscellaneous conditions; false positives <strong>are</strong><br />
r<strong>are</strong> in healthy individuals [4]. The use <strong>of</strong><br />
chicken, turkey and more recently human ‘O’<br />
RBCs has successfully reduced the number <strong>of</strong><br />
false positive results, as has the use <strong>of</strong> coloured<br />
gelatine or polymer particles, which has also<br />
greatly decreased the complexity <strong>of</strong> the test<br />
[2]. The TPPA test is an appropriate substitute<br />
<strong>for</strong> the microhaemagglutination assay<br />
(MHA-TP), as it is as sensitive as the fluorescent<br />
treponemal antibody absorbed (FTA-<br />
ABS) test <strong>for</strong> primary syphilis and as useful as<br />
the RPR <strong>for</strong> screening blood donors [7]. Furthermore<br />
it has been reported that sensitivity<br />
has increased due to the improved IgM binding<br />
capacity <strong>of</strong> sensitised gel particles.<br />
Enzyme Immuno Assay (EIA)<br />
The indirect competitive capture EIA, detecting<br />
IgG and/or IgM treponemal antibodies,<br />
has been developed by numerous laboratories.<br />
The tests have similar or higher sensitivity and
– February/March 2011 30 Microbiology<br />
specificity comp<strong>are</strong>d with the FTA-ABS and<br />
TPPA [6]. In addition they can be automated,<br />
facilitating the objective reading <strong>of</strong> results. The<br />
reader can be linked to the laboratory computer,<br />
which reduces the variation and subjectivity<br />
<strong>of</strong> manual reading. However, EIAs based<br />
on treponemal antigens, like other treponemal<br />
tests, give positive results throughout life even<br />
after successful completion <strong>of</strong> therapy. The<br />
sensitivity <strong>of</strong> EIA is also no greater than the<br />
TPHA <strong>for</strong> primary syphilis. The CDC recommends<br />
that if the EIA is used <strong>for</strong> screening, an<br />
RPR test should be per<strong>for</strong>med on all positive<br />
samples, and a second treponemal test, such as<br />
TPPA or FTA-ABS, should be used to confirm<br />
a positive result.<br />
Fluorescent Treponemal Antibody<br />
Absorption Test (FTA-Abs)<br />
This indirect fluorescent antibody test utilises<br />
fluorescent dye to detect antibodies against<br />
treponemal antigens. Serum or plasma is<br />
pretreated with absorbent to remove groupspecific<br />
treponemal antibodies. The FTA<br />
- Abs double staining test is a modified FTA-<br />
Abs which uses an additional counter stain<br />
to improve the reliability <strong>of</strong> the results. Even<br />
though it is highly sensitive, especially in early<br />
primary syphilis, it is less sensitive than other<br />
treponemal tests <strong>for</strong> detecting markers <strong>of</strong><br />
past infection [2]. The specificity <strong>of</strong> FTA-Abs<br />
is also lower than in other treponemal tests.<br />
False positives occur in approximately 1-2%<br />
<strong>of</strong> the normal population, mainly in patients<br />
with immune haemolytic anaemia, some viral<br />
infections and in narcotic addicts [2]. Furthermore<br />
an effective, specialised and qualitycontrolled<br />
microscope is required <strong>for</strong> the test.<br />
Immunoblotting<br />
This technique detects antibodies to individual<br />
T. pallidum proteins. Antibodies reacting to<br />
some <strong>of</strong> the treponemal antigens such as 15<br />
kDa, 17 kDa, 44.5 kDa and 47 kDa <strong>are</strong> diagnostic<br />
<strong>for</strong> acquired syphilis [2]. Either IgG or IgM<br />
antibodies <strong>are</strong> detected, which is useful <strong>for</strong> a<br />
confirmatory test [4, 6]. Recently recombinant<br />
antigens, in place <strong>of</strong> electrophoretically fractionated<br />
proteins, have improved the test, but it<br />
cannot be per<strong>for</strong>med in a small scale laboratory;<br />
the test is only available in selected laboratories.<br />
Rapid tests<br />
Rapid tests using treponemal antigen(s)<br />
coated on latex particles and nitrocellulose<br />
(ICT) strips <strong>are</strong> available <strong>for</strong> testing blood,<br />
serum or plasma. Such simple, rapid tests<br />
<strong>are</strong> more useful in the field, in resource-poor<br />
settings and in the physician’s <strong>of</strong>fice, as technical<br />
expertise and specialised instruments<br />
<strong>are</strong> not required. However rapid tests do not<br />
incorporate an internal Quality Control, so<br />
a periodic external Quality Control using<br />
laboratory-based tests is recommended [6].<br />
One such test is Span Diagnostics’s Signal –Tp<br />
ver. 2.0, an Immunodot test utilising a mixture<br />
<strong>of</strong> purified recombinant, treponemal antigens<br />
(47 kDa, 17 kDa), which <strong>are</strong> among the<br />
major immunoreactive antigens in Western<br />
Blot analysis and have shown great promise<br />
in the development <strong>of</strong> a rapid diagnostic test<br />
<strong>for</strong> syphilis [3,4]. Another test, Span Diagnostics’s<br />
Crystal- Tp, is based on an immunochromatographic<br />
technique which detects all<br />
major classes <strong>of</strong> antibodies i.e. IgG, IgM, IgA<br />
to treponemal antigens. A mixture <strong>of</strong> purified<br />
recombinant antigens is used- 15 kDa, 47 kDa<br />
and 17 kDa- which <strong>are</strong> major immunoreactive<br />
antigens in the Western Blot technique [3,4].<br />
These two tests have an inbuilt control dot/<br />
line. They <strong>are</strong> 100% sensitive when comp<strong>are</strong>d<br />
with a confirmed positive serum sample panel<br />
<strong>for</strong> anti treponemal antibodies, and 100% specific<br />
when comp<strong>are</strong>d with the TPHA.<br />
Practical utility <strong>of</strong> serological tests<br />
In the laboratory diagnosis <strong>of</strong> syphilis, it is most<br />
important to detect the antibody response<br />
with a screening test and confirm positive<br />
results using a confirmatory test. An ideal<br />
screening test should be simple, readily available,<br />
cost-effective, rapid, user-friendly, suitable<br />
<strong>for</strong> resource-poor situations and easily<br />
adapted <strong>for</strong> use with a large number <strong>of</strong> specimens.<br />
Sensitivity should be high, whereas the<br />
confirmatory test should have both high sensitivity<br />
and specificity, even at the cost <strong>of</strong> ease,<br />
economy and simplicity, to rule out all false<br />
positives without missing any positive samples.<br />
Although this combination provides an<br />
excellent screen <strong>for</strong> all stages <strong>of</strong> syphilis except<br />
<strong>for</strong> very early primary infections, when the<br />
treponemal test will not be positive, the cost<br />
should be considered. In collaboration with<br />
CDC, Span Diagnostics has developed world’s<br />
first dual-test in a flow-through <strong>for</strong>mat, the<br />
Signal Spirolipin, which detects reagin (i.e.<br />
nonspecific) as well as anti treponemal (i.e.<br />
specific) antibodies against a mixture <strong>of</strong> 47<br />
kDa and 17 kDa antigens in a single test. This<br />
can be used <strong>for</strong> screening and confirmation<br />
<strong>of</strong> syphilis in almost all disease stages without<br />
any prozone effect or false positives, and<br />
can also be used to monitor treatment with<br />
high specificity and sensitivity. Promising test<br />
results have been found in neuro-syphilis,<br />
congenital syphilis and in cases <strong>of</strong> syphilis/<br />
HIV coinfection. This test makes diagnosis<br />
quicker, more reliable, easier and more economical,<br />
without the need <strong>for</strong> specialised<br />
instruments and expertise. It is thus suitable<br />
<strong>for</strong> field and epidemiological studies. The Signal<br />
Spirolipin is a visual three dot assay with<br />
an inbuilt control dot to validate successful<br />
completion <strong>of</strong> the assay procedure; results <strong>are</strong><br />
available in 10 minutes.<br />
References<br />
1. CDC fact sheet, syphilis, 2008.<br />
2. Nester<strong>of</strong>f S. Serology, syphilis, RCPA Quality Programs Pty<br />
Limited, 2004.<br />
3. Egglestone SI and Turner AJL. Serological diagnosis <strong>of</strong> syphilis.<br />
Communicable disease and public health 2000; 3:158-62.<br />
4. Larsen SA, Steiner BM and Rudolph AH. Laboratory diagnosis<br />
and interpretation <strong>of</strong> tests <strong>for</strong> syphilis. Clinical Microbiology<br />
Reviews 1995; 8: 1-25.<br />
5. Muller I, Brade V et al. Is serological testing a reliable tool in<br />
laboratory diagnosis <strong>of</strong> syphilis? Meta-analysis <strong>of</strong> eight external<br />
Quality control surveys per<strong>for</strong>med by German Infection<br />
Serology Pr<strong>of</strong>iciency testing program, Journal <strong>of</strong> Clinical<br />
Microbiology 2006; 44:1335-1341.<br />
6. Ratnam S. The Laboratory diagnosis <strong>of</strong> syphilis. The Canadian<br />
Journal <strong>of</strong> Infectious disease and medical Microbiology 2005;<br />
16:45-51.<br />
7. Pope V et al. Comparison <strong>of</strong> serodia Treponema plallidum<br />
particle agglutination Captia Syphilis-G and SpiroTek regain<br />
II test with standard test technique <strong>for</strong> diagnosis <strong>of</strong> syphilis,<br />
Journal <strong>of</strong> Clinical Microbiology, 2001;38:2543-2548.<br />
The author<br />
Dr M. Patel<br />
SPAN DIAGNOSTICS LTD.<br />
Udhna, Surat,<br />
INDIA<br />
www.cli-online.com & search 25516<br />
Nova Biomedical increases<br />
manufacturing capability<br />
Nova Biomedical announced recently that, in<br />
response to rapid growth in its diabetes and<br />
whole blood point-<strong>of</strong>-c<strong>are</strong> testing products<br />
business, it has purchased an additional 7,500<br />
squ<strong>are</strong> metres <strong>of</strong> manufacturing/w<strong>are</strong>house<br />
facility in Billerica, MA, USA. According to<br />
Lou Borrelli, Nova Biomedical’s CFO, this<br />
additional state <strong>of</strong> the art manufacturing facility<br />
will ensure that the company’s manufacturing<br />
capabilities keep pace with the increasing<br />
demand <strong>for</strong> its StatStrip Hospital Glucose<br />
products as well as its Nova Max consumer<br />
diabetes products.<br />
One <strong>of</strong> the main drivers <strong>for</strong> Nova’s strong<br />
growth is the rapid adoption <strong>of</strong> its StatStrip<br />
Hospital Glucose Monitoring System. Since<br />
its inception just four years ago, StatStrip has<br />
become the fastest growing hospital glucose<br />
meter in the world. StatStrip uses a novel glucose<br />
test strip technology that measures haematocrit<br />
and other common interferences such<br />
as maltose, galactose, xylose, acetaminophen,<br />
ascorbic acid and oxygen, and eliminates erroneous<br />
glucose results caused by these interfering<br />
substances. StatStrip lab-like accuracy and<br />
freedom from interference has been validated<br />
in more than 50 published clinical studies<br />
worldwide, in a broad variety <strong>of</strong> critical c<strong>are</strong><br />
settings including ICU, Dialysis, NICU, OR,<br />
ED, and Tertiary C<strong>are</strong>. This remarkable rate <strong>of</strong><br />
StatStrip publications by some <strong>of</strong> the world’s<br />
leading hospitals, is testimony to the importance<br />
<strong>of</strong> this technology breakthrough <strong>for</strong> bedside<br />
glucose testing and suggests the reason <strong>for</strong><br />
its popularity.
Product News<br />
31<br />
– February/March 2011<br />
Human molecular<br />
karyotyping panel<br />
A multiplexed assay kit <strong>for</strong> human molecular<br />
karyotyping, the nCounter human<br />
karyotype panel provides a cost-effective<br />
way to monitor cell line quality and carry<br />
out cytogenetics research. With this kit,<br />
researchers can accurately quantify chromosome<br />
number and detect aneuploidy<br />
– the existence <strong>of</strong> fewer or more than the<br />
normal two chromosomes in a diploid<br />
genome. These assays <strong>are</strong> ideal <strong>for</strong> monitoring<br />
human-derived samples and cell<br />
lines <strong>for</strong> chromosomal abnormalities, and<br />
features less hands-on time than other<br />
products. Additional applications include<br />
the screening <strong>of</strong> human samples <strong>for</strong> clinical<br />
research and non-human cell lines <strong>for</strong><br />
human contamination as well as next-generation<br />
sequencing library quality control.<br />
NanoString Technologies, Inc<br />
Seattle, WA, USA<br />
www.cli-online.com & search 25502<br />
Legionella pneumophila<br />
monoclonal antibodies<br />
Legionella pneumophila is a gram negative<br />
organism, found in the natural environment,<br />
which can cause an infection <strong>of</strong><br />
the pulmonary alveolar macrophages, the<br />
condition also known as Legionnaire’s disease.<br />
Though there <strong>are</strong> 64 serogroups <strong>of</strong><br />
Legionella, 70-90% <strong>of</strong> cases <strong>of</strong> pneumonia<br />
<strong>are</strong> caused by serogroup 1 <strong>of</strong> L. pneumophila.<br />
Two new monoclonal antibodies react<br />
with the lipopolysaccharide (LPS) <strong>of</strong> all the<br />
serogroup 1 strains tested (11 strains). These<br />
antibodies can <strong>for</strong>m a pair <strong>for</strong> the detection<br />
<strong>of</strong> SG1 LPS from various samples.<br />
ViroStat, Inc<br />
Portland, ME, USA<br />
www.cli-online.com & search 25491<br />
Agar <strong>for</strong> rapid MRSA screening<br />
The newly improved Brilliance MRSA 2 Agar<br />
chromogenic medium saves valuable time <strong>for</strong><br />
infection control teams by allowing rapid and<br />
reliable screening <strong>for</strong> methicillin-resistant<br />
Staphylococcus aureus (MRSA). With accurate,<br />
easy-to-read results available in just 18<br />
hours, the agar enables prompt initiation<br />
<strong>of</strong> appropriate infection control measures<br />
to help minimise the opportunities <strong>for</strong> further<br />
transmission <strong>of</strong> MRSA. The enhanced<br />
<strong>for</strong>mulation ensures even easier interpretation<br />
<strong>of</strong> results. New inhibitory components<br />
in the medium further reduce the growth<br />
<strong>of</strong> non-target organisms, while a novel pink<br />
counter stain ensures that any organisms<br />
that do grow <strong>are</strong> easily distinguished from<br />
the distinctive blue MRSA colonies. The agar<br />
minimises false-positive results, even in low<br />
MRSA prevalence settings. This saves time<br />
and resources by reducing the need to reincubate<br />
plates and minimising confirmatory<br />
testing. Convenient<br />
and extremely<br />
easy to use, the<br />
agar is suitable <strong>for</strong><br />
inoculation direct<br />
from screening<br />
swabs, or it can be<br />
used to plate out an<br />
isolate or suspension.<br />
Thermo Fisher Scientific<br />
Basingstoke, Hants, UK<br />
www.cli-online.com & search 25496<br />
Dimeric antigen <strong>for</strong> greater<br />
specificity in Borrelia diagnostics<br />
An innovative dimeric Outer surface<br />
Proctein C (OspC_ antigen provides over<br />
30% higher specificity than conventional<br />
OspC in the serological diagnosis <strong>of</strong> Lyme<br />
disease. Antibodies against OspC <strong>are</strong> <strong>for</strong>med<br />
in as many as 90% <strong>of</strong> persons infected with<br />
Borrelia and represent the most important<br />
marker <strong>for</strong> early-stage borreliosis. Recent<br />
research has revealed that the biologically<br />
active <strong>for</strong>m <strong>of</strong> OspC is a homodimer. The<br />
recombinant OspC used in immunoassays is,<br />
however, typically produced in monomeric<br />
<strong>for</strong>m. To compensate <strong>for</strong> its correspondingly<br />
low sensitivity it is <strong>of</strong>ten coated at high<br />
concentrations, leading to numerous unspecific<br />
reactions. Now recombinant OspC has,<br />
<strong>for</strong> the first time, been produced in dimeric<br />
<strong>for</strong>m using state-<strong>of</strong>-the-art molecular biological<br />
methods. This dimeric antigen, OspC<br />
adv, has the same characteristics as the native<br />
dimeric protein. Its exceptionally high specificity<br />
minimises the risk <strong>of</strong> false-positive<br />
results, and it retains a high sensitivity. Moreover,<br />
in contrast to native protein which is<br />
difficult to isolate,<br />
this dimeric antigen<br />
can be produced<br />
using standardised<br />
methods, thus<br />
ensuring a highly<br />
consistent antigen<br />
quality. The antigen<br />
is now included in the Anti-Borrelia EURO-<br />
LINE-RN-AT immunoblot (IgG and IgM)<br />
from Euroimmun. This line blot system provides<br />
an extensive portfolio <strong>of</strong> diagnostically<br />
relevant antigens, including the important<br />
marker VlsE. Each antigen preparation is<br />
tailored to provide maximum sensitivity and<br />
specificity. The IgM blot features OspC adv<br />
from four different Borrelia species (afzelii,<br />
burgdorferi, garinii, spielmanii), encompassing<br />
all currently known human pathogenic<br />
species. The Anti-Borrelia immunoblot also<br />
includes immunoreactive membrane lipids<br />
— exclusive to this system — which further<br />
enhance the efficiency <strong>of</strong> the analysis, and is<br />
ideal <strong>for</strong> the second, confirmatory step <strong>of</strong> the<br />
recommended two-step strategy <strong>for</strong> serological<br />
Borrelia diagnostics. The system is also<br />
suitable <strong>for</strong> investigating CSF in the diagnosis<br />
<strong>of</strong> neuroborreliosis. The assay is easy to<br />
per<strong>for</strong>m and evaluate, and the entire analysis<br />
can be automated using specially developed<br />
devices and s<strong>of</strong>tw<strong>are</strong>.<br />
EUROIMMUN AG<br />
Luebeck, Germany<br />
www.cli-online.com & search 25500<br />
Targeted sequencing solution<br />
<strong>for</strong> FFPE samples<br />
An ultra-deep targeted sequencing system<br />
<strong>for</strong> fresh frozen and Formalin-Fixed Paraffin<br />
Embedded (FFPE) samples, the Deep-<br />
Seq FFPE solution is based on microdroplet-based<br />
single molecule PCR technology.<br />
Delivering high specificity, accurate quantification<br />
and unbiased allelic representation,<br />
it enables researchers to interrogate as many<br />
as 500 targets at up to 50,000-fold coverage<br />
across extensive collections <strong>of</strong> wellannotated<br />
clinical samples to discover r<strong>are</strong><br />
<strong>cancer</strong> and other disease-specific mutations<br />
that represent as little as one percent <strong>of</strong> a<br />
heterogeneous sample.<br />
RainDance Technologies, Inc<br />
Lexington, MA, USA<br />
www.cli-online.com & search 25489
– February/March 2011 32<br />
Product News<br />
Incubator with O 2<br />
and N 2<br />
control<br />
The MCO-19M CO 2<br />
incubator provides<br />
extremely accurate control <strong>of</strong><br />
the environment within the incubation<br />
chamber. CO 2<br />
concentration<br />
is measured using a dual infra red<br />
solid state sensor that is not affected<br />
by humidity or temperature changes<br />
when the incubator door is opened. In<br />
addition, the CO 2<br />
sensor remains calibrated<br />
continually without the need<br />
<strong>for</strong> timed recalibration procedures.<br />
O 2<br />
concentration is measured using a solid state zirconium sensor<br />
that is maintenance-free, thereby removing the need <strong>for</strong> constant<br />
recalibration. CO 2<br />
and O 2<br />
levels <strong>are</strong> controlled using a PID controller<br />
to ensure rapid recovery without excessive overshoot <strong>of</strong> the<br />
chosen gas-level set-points. A stable and uni<strong>for</strong>m temperature is<br />
provided within the chamber using Sanyo’s Direct Heat Air Jacket<br />
system, which is PID controlled to ensure rapid recovery after a<br />
door opening. The even distribution <strong>of</strong> temperature throughout<br />
focusonchangeHarrogate International Centre<br />
23–26 May 2011<br />
Harmonisation <strong>of</strong> Blood Sciences<br />
Emerging Technologies<br />
Cancer: Meeting the Needs <strong>of</strong><br />
the Patient<br />
Laboratory Automation<br />
Clinical Biochemistry and the<br />
Coroner<br />
Point <strong>of</strong> C<strong>are</strong> Testing<br />
Clinical Chemistry in the Age<br />
<strong>of</strong> Austerity<br />
Research in Clinical Biochemistry<br />
All day breakfast workshops<br />
www.focus-acb.org.uk<br />
the chamber contributes to the shelf-to-shelf reproducibility <strong>of</strong><br />
conditions. The interior <strong>of</strong> the chamber is manufactured from<br />
InCu saFe, a copper-enriched stainless steel antimicrobial alloy,<br />
which inhibits the growth <strong>of</strong> fungi, mycoplasma and bacteria. For<br />
critical applications the SafeCell UV system automatic decontamination<br />
systems can be incorporated; this optional UV Illuminated<br />
air duct automatically maintains contamination-free air<br />
and humidity within the chamber. For applications which require<br />
additional decontamination, the hydrogen peroxide decontamination<br />
system is extremely effective and fast: a complete cycle only<br />
takes 130 minutes. This system is also safe, since the H 2<br />
O 2<br />
vapour<br />
is contained within the incubator and is broken down to water and<br />
oxygen at the end <strong>of</strong> the cycle. The door interlock and alarm also<br />
ensure that the system is safe.<br />
Sanyo BiomedicaL<br />
Etten-Leur, The Netherlands<br />
www.cli-online.com & search 25512<br />
Midkine ELISA<br />
Midkine (MK) — also<br />
known as neurite growth<br />
promoting factor 2<br />
(NEGF-2) — is a cytokine<br />
that is expressed during<br />
embryonic development.<br />
In healthy adults MK is<br />
expressed at only low levels.<br />
However, MK levels <strong>are</strong> found to be elevated in the blood and<br />
urine <strong>of</strong> patients with carcinomas including oesophageal, stomach,<br />
colon, pancreatic, thyroid, lung, urinary, hepatocellular, neuroblastoma,<br />
glioblastoma, and Wilm´s tumour. MK levels can be<br />
measured in the early stage <strong>of</strong> <strong>cancer</strong> development, making MK<br />
an optimal marker <strong>for</strong> screening and preventive healthc<strong>are</strong>. The<br />
determination <strong>of</strong> MK in blood even detects organ-located solid<br />
tumour malignancy. High MK levels <strong>are</strong> associated with poor<br />
prognosis in some types <strong>of</strong> <strong>cancer</strong>. The combination <strong>of</strong> MK detection<br />
together with established oncologic markers improves <strong>cancer</strong><br />
diagnosis. The Human Midkine ELISA kit extends BioVendor’s<br />
portfolio <strong>of</strong> diagnostic kits <strong>for</strong> oncology. Suitable <strong>for</strong> serum and<br />
plasma samples, the 96 well-microtitre plate <strong>for</strong>mat is suitable <strong>for</strong><br />
use with standard ELISA equipment or robotic systems.<br />
Biovendor<br />
Modrice, The Czech Republic<br />
www.cli-online.com & search 25511<br />
Clinical chemistry analyser<br />
Designed <strong>for</strong> small- to mid-sized<br />
hospitals and laboratories, the<br />
BioMajesty 6010 is a very compact<br />
fully automatic chemical<br />
analyser which can handle up to<br />
1200 tests per hour. With 43 reagents<br />
and 84 sample positions,<br />
it provides the flexibility needed<br />
<strong>for</strong> routine use. Both photometric<br />
and immunoturbidimetric<br />
assays can be per<strong>for</strong>med as well as Na, K and Cl electrolyte<br />
determination using indirect ISE methods. Special emphasis has<br />
been given to the s<strong>of</strong>tw<strong>are</strong>, which combines a high degree <strong>of</strong> user
Product News<br />
33<br />
– February/March 2011<br />
friendliness with optimally secure results.<br />
An integrated on-board haemolysis function<br />
optimises HbA1c determination. In<br />
addition, only very small sample volumes<br />
<strong>are</strong> required, so it is ideal in paediatric and<br />
geriatric settings. The system has readyto-use<br />
reagents with excellent on-board<br />
stability; and reagent consumption is very<br />
low.<br />
DiaSys Diagnostic Systems<br />
GmbH<br />
Holzheim, Germany<br />
www.cli-online.com & search 25483<br />
Xylene-free tissue<br />
processing<br />
Traditionally xylene<br />
has been used as<br />
a clearing agent in<br />
tissue processing<br />
<strong>for</strong> many years, primarily<br />
because <strong>of</strong><br />
its miscibility with<br />
both alcohol and<br />
wax, while very effectively clearing the tissue<br />
<strong>of</strong> alcohol. However, xylene also exposes<br />
lab personnel to hazardous fumes. Fortunately<br />
this is no longer an issue with Tissue-<br />
Tek Tissue-Clear, which is a non-toxic, nonflammable,<br />
odourless and biodegradable<br />
(thus environmentally-friendly), substitute<br />
<strong>for</strong> xylene. It is also compatible with a common<br />
mounting medium, and its biodegradable<br />
and non-hazardous properties allow<br />
<strong>for</strong> easy disposal (depending on permission<br />
by appropriate local authorities). Substituting<br />
xylene by Tissue-Tek Tissue-Clear in a<br />
traditional processing programme on a Tissue-Tek<br />
VIP 6 will not jeopardise specimen<br />
integrity or quality. Whether a laboratory<br />
chooses to use a long or short programme<br />
<strong>for</strong> processing, lab personnel no longer have<br />
to be subjected to hazardous xylene fumes.<br />
Sakura Finetek Europe B.V.<br />
Alphen Aan Den Rijn, The Netherlands<br />
www.cli-online.com & search 25498<br />
NGAL test <strong>for</strong> diagnostic use<br />
NGAL is a novel biomarker <strong>for</strong> diagnosing<br />
acute kidney injury (AKI). The key advantage<br />
<strong>of</strong> NGAL is that it responds earlier than<br />
other renal status markers such as serum creatinine<br />
and shows a proportionate response<br />
to injury. NGAL there<strong>for</strong>e provides a new<br />
way to identify patients at risk <strong>of</strong> developing<br />
potentially severe acute kidney injury (AKI)<br />
24-72 hours be<strong>for</strong>e the problem would otherwise<br />
be detected. The NGAL Test from Bio-<br />
Porto, previously available <strong>for</strong> research use<br />
and successfully tested in selected hospitals in<br />
Europe, the USA and Southeast Asia, is now<br />
CE-marked and available <strong>for</strong> use in Europe<br />
<strong>for</strong> early diagnosis <strong>of</strong> acute kidney injury. It<br />
will soon be possible to obtain The NGAL<br />
Test <strong>for</strong> diagnostic use in approximately 40<br />
countries. Using only a few drops <strong>of</strong> plasma<br />
or urine the test provides results in just 10<br />
minutes and thus addresses the widespread<br />
demand <strong>for</strong> urgent NGAL determination.<br />
Designed to run on open channels <strong>of</strong> chemistry<br />
analysers from numerous manufacturers,<br />
most laboratories thus have a convenient<br />
and easy way to measure NGAL.<br />
BioPorto Diagnostics A/S<br />
Gent<strong>of</strong>te, Denmark<br />
www.cli-online.com & search 25488<br />
Rivaroxaban calibrators and<br />
controls <strong>for</strong> monitoring therapy<br />
Rivaroxaban is a<br />
new oral anticoagulant,<br />
developed<br />
by Bayer Healthc<strong>are</strong><br />
and sold under<br />
the trade name<br />
<strong>of</strong> X<strong>are</strong>lto. It is a<br />
direct factor Xa<br />
inhibitor approved<br />
in more than 80<br />
countries <strong>for</strong> the<br />
prevention <strong>of</strong> VTE after hip or knee surgery.<br />
Rivaroxaban is expected to be approved in<br />
the near future <strong>for</strong> other indications such<br />
as stroke prevention in patients with atrial<br />
fibrillation, thus making it a very useful and<br />
important anticoagulant. The STA-Rivaroxaban<br />
Calibrator & Control solution is<br />
designed <strong>for</strong> the determination <strong>of</strong> rivaroxaban<br />
concentration. Including rivaroxaban<br />
calibrators and controls, this solution can<br />
be used in two methods <strong>for</strong> different clinical<br />
needs and laboratory requirements. These<br />
<strong>are</strong> respectively the PT-derived method<br />
(STA-Neoplastine CI Plus), a cost effective<br />
global test <strong>for</strong> screening purposes, and the<br />
Anti-Xa method (STA-Liquid Anti-Xa),<br />
which is insensitive to analytical and biological<br />
variables and has a wide working range<br />
<strong>for</strong> specific and more sensitive dosage determination.<br />
Results <strong>are</strong> expressed in ng/mL<br />
<strong>of</strong> rivaroxaban. Reagents <strong>are</strong> barcoded <strong>for</strong><br />
optimal ease <strong>of</strong> handling and traceability,<br />
and methods can be fully automated on the<br />
STA line, with dedicated test setups. Results<br />
<strong>are</strong> available in a few minutes, sso the system<br />
is ideal <strong>for</strong> STAT sample requirements.<br />
Diagnostica Stago<br />
Asnières sur Seine, France<br />
www.cli-online.com & search 25482<br />
Treponema pallidum IgG<br />
test system<br />
Syphilis is a bacterial infection that is<br />
usually sexually transmitted, but may<br />
also be passed from an infected mother<br />
to her unborn child. Syphilis is a curable<br />
sexually transmitted disease (STD) which,<br />
however if left untreated can eventually<br />
lead to irreversible damage to the heart<br />
and nervous system. Despite the existence<br />
<strong>of</strong> effective prevention measures, the<br />
disease remains a global problem with an<br />
estimated 12 million people infected each<br />
year. The ZEUS ELISA IgG test system<br />
allows the qualitative detection <strong>of</strong> specific<br />
human IgG class antibodies to Treponema<br />
pallidum in human sera. The presence <strong>of</strong><br />
antibodies to T. pallidum specific antigen,<br />
in conjunction with non-treponemal<br />
laboratory tests and clinical findings, may<br />
aid in the diagnosis <strong>of</strong> syphilis infection.<br />
Together with the company’s AtheNA<br />
Multi-Lyte Treponema pallidum IgG Plus<br />
Test System, multiple testing solutions<br />
<strong>for</strong> the qualitative detection <strong>of</strong> specific<br />
human IgG class antibodies to T. pallidum<br />
in human sera <strong>are</strong> now available.<br />
Zeus scientific<br />
Raritan, NJ, USA<br />
www.cli-online.com & search 25513<br />
PCR-ready human genomic<br />
DNA extraction<br />
It is now possible<br />
to extract and<br />
purify human<br />
genomic DNA<br />
from whole<br />
blood much<br />
faster than with<br />
a spin column<br />
<strong>for</strong> use in genetic<br />
testing, pharmacogenomics<br />
and<br />
<strong>for</strong>ensic applications.<br />
Using an Eppendorf epMotion<br />
automated pipetting station, Akonni<br />
TruTip delivers with the simple push <strong>of</strong><br />
a button inhibitor-free, PCR-ready DNA<br />
up to five times faster than ‘gold standard’<br />
spin columns. Alternatively one to<br />
eight ultra-rapid manual extractions can<br />
be per<strong>for</strong>med with TruTip and a Rainin<br />
EDP 3Plus single- or multi-channel<br />
pipette, in as few as four minutes. Yields<br />
and purity <strong>are</strong> comparable to those<br />
obtained using gold standard kits.<br />
Akonni Biosystems<br />
Frederick, MD, USA<br />
www.cli-online.com & search 25481
– February/March 2011 34<br />
Product News<br />
STAT immunoassays <strong>for</strong> cardiac<br />
biomarker testing<br />
Roche has introduced a complete battery <strong>of</strong><br />
STAT immunoassays <strong>for</strong> cardiac biomarker<br />
testing on the cobas 6000 analyser series, the<br />
integrated system designed <strong>for</strong> diagnostic<br />
labs with medium testing volumes. With a<br />
nine-minute duration, the assays <strong>are</strong> faster<br />
than any other cardiac immunoassay tests<br />
currently available on an integrated plat<strong>for</strong>m<br />
and enable labs to deliver results to<br />
doctors treating cardiac patients in about<br />
half the time <strong>of</strong> standard Roche tests. The<br />
tests include troponin T, CK-MB, myoglobin<br />
and NT-proBNP, and <strong>are</strong> virtually<br />
equivalent to the company’s 18-minute tests<br />
in per<strong>for</strong>mance, precision and sensitivity.<br />
Roche diagnostics<br />
Mannheim, Germany<br />
www.cli-online.com & search 25485<br />
Immun<strong>of</strong>luorescence<br />
laboratory s<strong>of</strong>tw<strong>are</strong><br />
A complete<br />
system <strong>for</strong> the<br />
management <strong>of</strong><br />
autoimmune IF<br />
lab procedures,<br />
the i-mLS is an<br />
extremely userfriendly<br />
s<strong>of</strong>tw<strong>are</strong><br />
that provides a high level <strong>of</strong> control <strong>of</strong> all<br />
aspects <strong>of</strong> autoimmune IF testing. Designed<br />
to be the ideal companion <strong>for</strong> the I-mLD<br />
microscope, the s<strong>of</strong>tw<strong>are</strong> enables users to<br />
capture and store microscope images and to<br />
create a customised image catalogue <strong>for</strong> use<br />
as a reference. The s<strong>of</strong>tw<strong>are</strong> also allows easy<br />
result reporting and the addition <strong>of</strong> comments<br />
from the analyst, which can be introduced<br />
either into the basic system or into<br />
a report <strong>for</strong>mat. In addition, the s<strong>of</strong>tw<strong>are</strong><br />
enables the inclusion <strong>of</strong> additional in<strong>for</strong>mation<br />
such as clinical comments and images<br />
<strong>of</strong> patient tests, the consultation <strong>of</strong> results<br />
by patient, test or session, as well as communication<br />
with the LIS. When connected<br />
to the i-Pro immun<strong>of</strong>luorescence processor,<br />
the i-mLS s<strong>of</strong>tw<strong>are</strong> can import current session<br />
in<strong>for</strong>mation, read results at the microscope<br />
and then export data back to the i-Pro<br />
in<strong>for</strong>mation on a new working session with<br />
new or repeat test request. The system also<br />
allows laboratory managers to maintain<br />
traceability <strong>of</strong> reagents used in all tests per<strong>for</strong>med<br />
on the i-Pro and to remotely access<br />
stored results from their own <strong>of</strong>fice.<br />
BioSystems<br />
Barcelona, Spain<br />
www.cli-online.com & search 25484<br />
Platelet disfunction test system<br />
The next-generation <strong>of</strong> Siemens’ best-in-class<br />
technology to detect inherited, acquired, and<br />
drug-induced platelet dysfunction, the new<br />
INNOVANCE PFA 200 system has userfriendly<br />
updates including a colour LCD<br />
touchscreen to access detailed patient and<br />
result in<strong>for</strong>mation, a barcode reader <strong>for</strong> digital<br />
patient result tracking and LIS connection,<br />
and a USB port to archive stored data. The<br />
system also has multiple user-friendly s<strong>of</strong>tw<strong>are</strong><br />
updates, including new s<strong>of</strong>tw<strong>are</strong> that<br />
supports closure curve illustrations <strong>for</strong> use in<br />
scientific studies. Results, which <strong>are</strong> avaiable<br />
in 4-8 minutes, allow rapid comprehensive<br />
bleeding assessment. The system carries out<br />
collagen/EPI and collagen/ADP tests and the<br />
company’s latest addition, the P2Y test <strong>for</strong><br />
detection <strong>of</strong> platelet P2Y12-receptor blockades<br />
in patients.<br />
Siemens Medical Solutions<br />
Diagnostics<br />
Tarrytown, NY, USA<br />
www.cli-online.com & search 25514<br />
Vitamin D control<br />
Now available throughout the European<br />
Union, Fujirebio Diagnostics’ Vitamin D<br />
Control contains both 25(OH) Vitamin D2<br />
and 25(OH) Vitamin D3, and is intended<br />
<strong>for</strong> use as a quantitative, assayed serum<br />
control. The control has excellent stability,<br />
<strong>value</strong> assignment across plat<strong>for</strong>ms and<br />
clinically relevant levels, enabling laboratories<br />
to monitor the per<strong>for</strong>mance <strong>of</strong> their<br />
vitamin D assays.<br />
Fujirebio diagnostics<br />
Malvern, PA, USA<br />
www.cli-online.com & search 25487<br />
Calendar <strong>of</strong> events<br />
May 7-10, 2011<br />
21st ECCMID / 27th ICCs<br />
Milan, Italy<br />
Tel. +41 61 686 77 11<br />
Fax +41 61 686 77 88<br />
e-mail: eccmid@escmid.org<br />
www.eccmid-icc2011.org<br />
May 9-13, 2011<br />
4th International Congress <strong>of</strong><br />
Myology<br />
Lille, France<br />
Tel. +33 4 78 176 276<br />
http://myology2011.org/<br />
index_us.html<br />
May 13-15, 2011<br />
XIIth International Congress <strong>of</strong><br />
Paediatric Laboratory Medicine<br />
(ICPLM)<br />
Berlin, Germany<br />
Tel. +39 0266802323<br />
e-mail: icplm2011@mzcongressi.com<br />
www.icplm2011.org/<br />
May 15-19, 2011<br />
IFCC-Worldlab-Euromedlab<br />
Berlin 2011 Congress<br />
Berlin, Germany<br />
Tel. +39 02 66802323<br />
Fax +39 02 6686699<br />
e-mail: info@berlin2011.org<br />
www.berlin2011.org<br />
May 23-26, 2011<br />
FOCUS 2011<br />
Harrogate, UK<br />
Tel. +44 141 434 1500<br />
Fax +44 141 434 1519<br />
e-mail: focus2011@meetingmakers.co.uk<br />
www.focus-acb.org.uk<br />
May 24-27, 2011<br />
Hospitalar 2011<br />
São Paulo, Brazil<br />
www.hospitalar.com/ingles/<br />
June 25-29, 2011<br />
10th World Congress on<br />
Inflammation<br />
Paris, France<br />
Tel. 33 1 53 85 82 71<br />
Fax 33 1 53 85 82 83<br />
Email:<br />
info@inflammation2011.com<br />
www.inflammation2011.com<br />
July 17-20, 2011<br />
6th IAS Conference on HIV<br />
Pathogenesis, Treatment and<br />
Prevention<br />
Rome, Italy<br />
www.ias2011.org<br />
July 24-28, 2011<br />
2011 AACC Annual Meeting<br />
Atlanta, GA, USA<br />
www.aacc.org/<br />
events/2011am/<br />
September 21-24, 2011<br />
14th Annual Meeting <strong>of</strong> the<br />
European Society <strong>for</strong> Clinical<br />
Virology (ESCV)<br />
Funchal, Madeira, Portugal<br />
www.escv.org/meetings/meetings.asp<br />
October 2-6, 2011<br />
12th International Congress <strong>of</strong><br />
Therapeutic Drug Monitoring<br />
and Clinical Toxicology<br />
Stuttgart, Germany<br />
Tel. +49 711 8931 636<br />
Fax +49 711 8931 370<br />
e-mail: info@iatdmct2011.de<br />
www.iatdmct2011.de<br />
October 15 – 16, 2011<br />
The Lancet / ESCMID Conference<br />
on Healthc<strong>are</strong>-Associated<br />
Infections and Antimicrobial<br />
Resistance<br />
Beijing, China<br />
Tel. +86 21 61333077<br />
Fax +86 21 52980210<br />
e-mail: summitenquiry@elsevier.com<br />
October 24–26, 2011<br />
ESCMID Conference on<br />
Diagnosing Infectious Diseases:<br />
Future and Innovation<br />
Venice, Italy<br />
Tel. +39 041 52 62 530<br />
Fax +39 041 52 71 129<br />
e-mail: ico@icorganization.it<br />
www.escmid.org<br />
For more events see:<br />
www.cli-online.com/events/<br />
Dates and descriptions <strong>of</strong> future<br />
events have been obtained from<br />
<strong>of</strong>ficial industrial sources. CLi cannot<br />
be held responsible <strong>for</strong> errors,<br />
changes or cancellations.
Who can really help me grow?<br />
Only Siemens has the innovative solutions your lab needs<br />
to reach the top and the vision to keep you there.<br />
Planning <strong>for</strong> your future starts with choosing the right diagnostics partner today. Siemens provides comprehensive and<br />
customizable solutions so laboratorians and clinicians can improve productivity every day. And, with a 130-year tradition<br />
<strong>of</strong> innovation, you can trust Siemens to stay on the leading edge <strong>of</strong> emerging trends and technologies, so together we<br />
can set a new standard in patient c<strong>are</strong> <strong>for</strong> years to come. www.siemens.com/diagnostics<br />
Answers <strong>for</strong> life.<br />
A91DX-9105-A1-4A00<br />
© 2011 Siemens Healthc<strong>are</strong> Diagnostics. All rights reserved.<br />
www.cli-online.com & search 25418
www.cli-online.com & search 25463