

Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
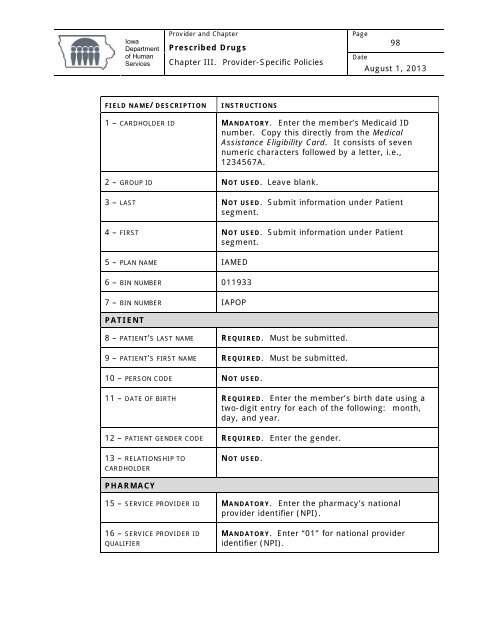
<strong>Iowa</strong><strong>Department</strong><strong>of</strong> <strong>Human</strong>Services<strong>Provider</strong> and Chapter<strong>Prescribed</strong> <strong>Drugs</strong>Chapter III. <strong>Provider</strong>-Specific PoliciesPage98DateAugust 1, 2013FIELD NAME/DESCRIPTIONINSTRUCTIONS1 – CARDHOLDER ID MANDATORY. Enter the member’s Medicaid IDnumber. Copy this directly from the MedicalAssistance Eligibility Card. It consists <strong>of</strong> sevennumeric characters followed by a letter, i.e.,1234567A.2 – GROUP ID NOT USED. Leave blank.3 – LAST NOT USED. Submit information under Patientsegment.4 – FIRST NOT USED. Submit information under Patientsegment.5 – PLAN NAME IAMED6 – BIN NUMBER 0119337 – BIN NUMBER IAPOPPATIENT8 – PATIENT’S LAST NAME REQUIRED. Must be submitted.9 – PATIENT’S FIRST NAME REQUIRED. Must be submitted.10 – PERSON CODE NOT USED.11 – DATE OF BIRTH REQUIRED. Enter the member’s birth date using atwo-digit entry for each <strong>of</strong> the following: month,day, and year.12 – PATIENT GENDER CODE REQUIRED. Enter the gender.13 – RELATIONSHIP TOCARDHOLDERNOT USED.PHARMACY15 – SERVICE PROVIDER ID MANDATORY. Enter the pharmacy’s nationalprovider identifier (NPI).16 – SERVICE PROVIDER IDQUALIFIERMANDATORY. Enter “01” for national provideridentifier (NPI).













