

Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
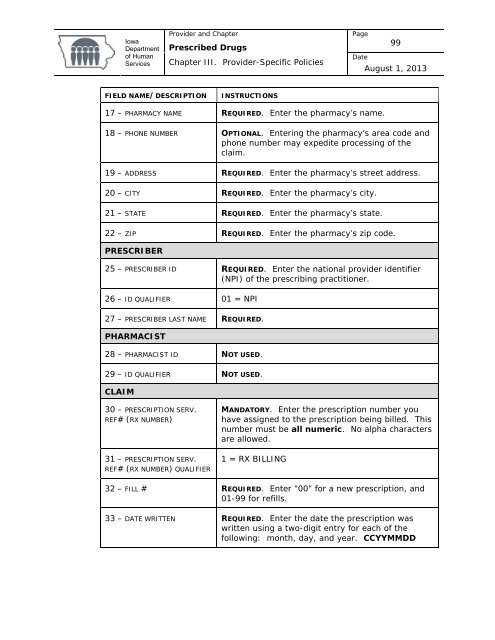
<strong>Iowa</strong><strong>Department</strong><strong>of</strong> <strong>Human</strong>Services<strong>Provider</strong> and Chapter<strong>Prescribed</strong> <strong>Drugs</strong>Chapter III. <strong>Provider</strong>-Specific PoliciesPage99DateAugust 1, 2013FIELD NAME/DESCRIPTIONINSTRUCTIONS17 – PHARMACY NAME REQUIRED. Enter the pharmacy’s name.18 – PHONE NUMBER OPTIONAL. Entering the pharmacy’s area code andphone number may expedite processing <strong>of</strong> theclaim.19 – ADDRESS REQUIRED. Enter the pharmacy’s street address.20 – CITY REQUIRED. Enter the pharmacy’s city.21 – STATE REQUIRED. Enter the pharmacy’s state.22 – ZIP REQUIRED. Enter the pharmacy’s zip code.PRESCRIBER25 – PRESCRIBER ID REQUIRED. Enter the national provider identifier(NPI) <strong>of</strong> the prescribing practitioner.26 – ID QUALIFIER 01 = NPI27 – PRESCRIBER LAST NAME REQUIRED.PHARMACIST28 – PHARMACIST ID NOT USED.29 – ID QUALIFIER NOT USED.CLAIM30 – PRESCRIPTION SERV.REF# (RX NUMBER)31 – PRESCRIPTION SERV.REF# (RX NUMBER) QUALIFIERMANDATORY. Enter the prescription number youhave assigned to the prescription being billed. Thisnumber must be all numeric. No alpha charactersare allowed.1 = RX BILLING32 – FILL # REQUIRED. Enter “00” for a new prescription, and01-99 for refills.33 – DATE WRITTEN REQUIRED. Enter the date the prescription waswritten using a two-digit entry for each <strong>of</strong> thefollowing: month, day, and year. CCYYMMDD













