

Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
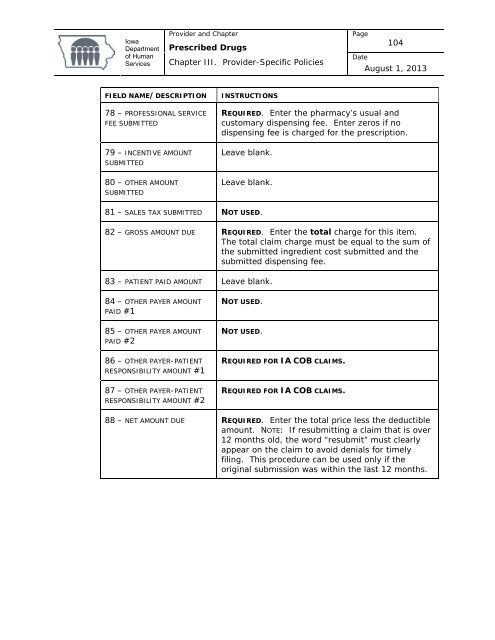
<strong>Iowa</strong><strong>Department</strong><strong>of</strong> <strong>Human</strong>Services<strong>Provider</strong> and Chapter<strong>Prescribed</strong> <strong>Drugs</strong>Chapter III. <strong>Provider</strong>-Specific PoliciesPage104DateAugust 1, 2013FIELD NAME/DESCRIPTION78 – PROFESSIONAL SERVICEFEE SUBMITTED79 – INCENTIVE AMOUNTSUBMITTED80 – OTHER AMOUNTSUBMITTEDINSTRUCTIONSREQUIRED. Enter the pharmacy’s usual andcustomary dispensing fee. Enter zeros if nodispensing fee is charged for the prescription.Leave blank.Leave blank.81 – SALES TAX SUBMITTED NOT USED.82 – GROSS AMOUNT DUE REQUIRED. Enter the total charge for this item.The total claim charge must be equal to the sum <strong>of</strong>the submitted ingredient cost submitted and thesubmitted dispensing fee.83 – PATIENT PAID AMOUNT Leave blank.84 – OTHER PAYER AMOUNTPAID #185 – OTHER PAYER AMOUNTPAID #286 – OTHER PAYER-PATIENTRESPONSIBILITY AMOUNT #187 – OTHER PAYER-PATIENTRESPONSIBILITY AMOUNT #2NOT USED.NOT USED.REQUIRED FOR IA COB CLAIMS.REQUIRED FOR IA COB CLAIMS.88 – NET AMOUNT DUE REQUIRED. Enter the total price less the deductibleamount. NOTE: If resubmitting a claim that is over12 months old, the word “resubmit” must clearlyappear on the claim to avoid denials for timelyfiling. This procedure can be used only if theoriginal submission was within the last 12 months.













