

Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...
Prescribed Drugs Provider Manual - Iowa Department of Human ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
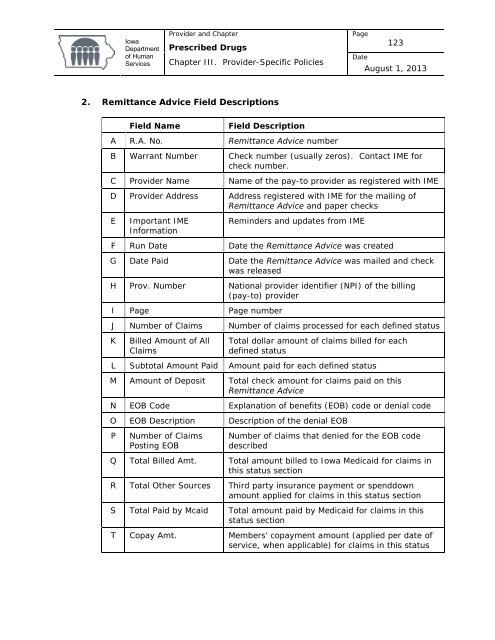
<strong>Iowa</strong><strong>Department</strong><strong>of</strong> <strong>Human</strong>Services<strong>Provider</strong> and Chapter<strong>Prescribed</strong> <strong>Drugs</strong>Chapter III. <strong>Provider</strong>-Specific PoliciesPage123DateAugust 1, 20132. Remittance Advice Field DescriptionsField NameField DescriptionA R.A. No. Remittance Advice numberB Warrant Number Check number (usually zeros). Contact IME forcheck number.C <strong>Provider</strong> Name Name <strong>of</strong> the pay-to provider as registered with IMED <strong>Provider</strong> Address Address registered with IME for the mailing <strong>of</strong>Remittance Advice and paper checksEImportant IMEInformationReminders and updates from IMEF Run Date Date the Remittance Advice was createdG Date Paid Date the Remittance Advice was mailed and checkwas releasedH Prov. Number National provider identifier (NPI) <strong>of</strong> the billing(pay-to) providerI Page Page numberJ Number <strong>of</strong> Claims Number <strong>of</strong> claims processed for each defined statusKBilled Amount <strong>of</strong> AllClaimsTotal dollar amount <strong>of</strong> claims billed for eachdefined statusL Subtotal Amount Paid Amount paid for each defined statusM Amount <strong>of</strong> Deposit Total check amount for claims paid on thisRemittance AdviceN EOB Code Explanation <strong>of</strong> benefits (EOB) code or denial codeO EOB Description Description <strong>of</strong> the denial EOBPNumber <strong>of</strong> ClaimsPosting EOBNumber <strong>of</strong> claims that denied for the EOB codedescribedQ Total Billed Amt. Total amount billed to <strong>Iowa</strong> Medicaid for claims inthis status sectionR Total Other Sources Third party insurance payment or spenddownamount applied for claims in this status sectionS Total Paid by Mcaid Total amount paid by Medicaid for claims in thisstatus sectionT Copay Amt. Members’ copayment amount (applied per date <strong>of</strong>service, when applicable) for claims in this status













