PROSTHODONTICS - American College of Prosthodontists
PROSTHODONTICS - American College of Prosthodontists
PROSTHODONTICS - American College of Prosthodontists

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
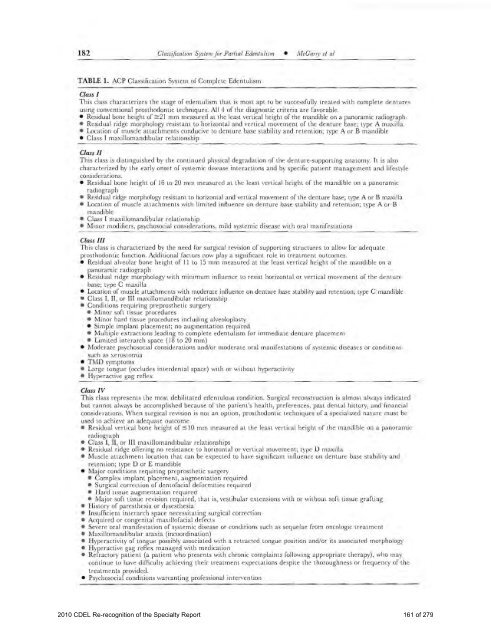
182 Classification System for Partial Edentulism • M cGarry et alTABLE 1. ACP Class ification System <strong>of</strong> Complete EdentulismClass IThis class characterizes the stage <strong>of</strong> edentulism that is most apt to be successfully treated with complete denturesusing conventional prosthodontic techniques. All 4 <strong>of</strong> the diagnostic criteria are favorable.• Residual bone height <strong>of</strong> :2:21 mm measured at the least vertical height <strong>of</strong> the mandible on a panoramic radiograph.• Residual ridge morphology resistant to horizontal and vertical movement <strong>of</strong> the denture base; type A maxilla.• Location <strong>of</strong> muscle attachments conducive to denture base stability and retention; type A or B mandible• Class I maxilloma ndibular relationshipClass IIThis class is distingui shed by the continuEd physical degradation <strong>of</strong> the denture-supporting anatomy. It is alsocharacterized by the early onset <strong>of</strong> systemic disease interactions and by specific patient management a nd lifestyleconsiderations.• Residual bone height <strong>of</strong> ]6 to 20 mm measured at the least vertica l height <strong>of</strong> the mandible on a panoramicradiograph• Residual ridge morphology resistant to horizontal and vertical movement <strong>of</strong> the denture base; type A or B maxilla• Location <strong>of</strong> muscle attachments with limited influence on denture base stability and re tention; type A or Bmandible• Class I maxilloma ndibular relationship• Minor modifiers, psyc hosocial considerations, mild systemic disease with oral manifestationsClass IIIThis class is cha racterized by the need for surgical revision <strong>of</strong> supporting structures to a llow for adequateprosthodontic function. Additional factors now play a significant role in treatment outcomes.• Res idual al veol ar bone height <strong>of</strong> II to 15 mm measured at the least vertical height <strong>of</strong> the mandible on apanoramic radiograph• Residual ridge morphology with minimum influ ence to resist horizontal or vertical movement <strong>of</strong> the denturebase; type C maxilla• Location <strong>of</strong> muscle attachments with moderate influence on denture base stability and retention; type C mandible• Class I, II, or III maxillomandibular relationship• Conditions requiring preprosthetic surgery• Minor s<strong>of</strong>t tiSSUE procedures• Minor hard tissue procedures including alveoloplasty• Simple implant placement; no augmentation required• Multiple extractions le ading to complete eclentulism for immediate denture placement• Limited interarch space (18 to 20 mm)• Moderate psychosocial considerations and/or moderate oral manifestations <strong>of</strong> systemic diseases or conditionssuch as xerostomia• Twill symptoms• Large tongue (occludes interdental space) with or without hyperactivity• H yperactive gag refl exClass IVThis class represents the most debilitated edentulolls condition. Surgical reconstruction is almost always indicatedbut cannot always be acco mplished because <strong>of</strong> the pati ent's health, preferences, past dental histo ry, and financialconsiderations. When surgical revision is not an option, prosthodontic techniques <strong>of</strong> a specialized nature must beused to achieve an adequate outcome.• Residual vertical bone height <strong>of</strong>:510 mm measured at the least vertical height <strong>of</strong> the mandible 01) a panoramicradiograph• Class I , II, or III maxillomandibular relationships• Res idual ridge <strong>of</strong>Tering no resistance to horizontal or vertical movement; type D maxilla• Muscle attachment location that can be expected to have significant influence on denture baSE stability andretention; type D or E mandible• Major conditions requiring preprosthetic surgery• Complex implant placement, augmentation requi red• Surgical correction <strong>of</strong> dent<strong>of</strong>acial deformities required• Hard tissue augmen tation required• jYIajor s<strong>of</strong>t tissue revision required, that is, vestibular extensions with or witbout s<strong>of</strong>t tissue grafting• History <strong>of</strong> paresthesia or dysesthesia• Insufficient interarch space necess itating surgical correction• Acquired or congenital maxill<strong>of</strong>acial defects• Seve re oral. manifesta tion <strong>of</strong> systemic disease or conditions such as sequelae from oncologic treatment• Maxillomandibular ataxia (incoordination)• H yperactivity <strong>of</strong> tong ue possi bl y associated with a retracted tongue position and/or its associated morphology• H ype ractive gag reflex managed "rith medication• Refractory patient (a patient wbo prese nts with chronic complaints foll owing appropriate therapy), who maycontinue to have difficulty achi eving their treatment expectations despite the thoroughness or frequency <strong>of</strong> thetreatments provided.• Psychosocial conditions warranting pr<strong>of</strong>essional intervention2010 CDEL Re-recognition <strong>of</strong> the Specialty Report 161 <strong>of</strong> 279