INDICATORS
ECHIM Final Report
ECHIM Final Report

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Typically, national health information systems compile data from several sources<br />
based on national data gathering routines. These data sources regularly produce a large<br />
amount of data that are usually distributed to a number of agencies and institutes.<br />
The processing and analysis is performed in diverse organisational structures, usually<br />
under the responsibility of different authorities. The integration and rationalisation of<br />
this fragmented information and the underlying distributed data sources is one of the<br />
key issues that has to be resolved in the development of a national health information<br />
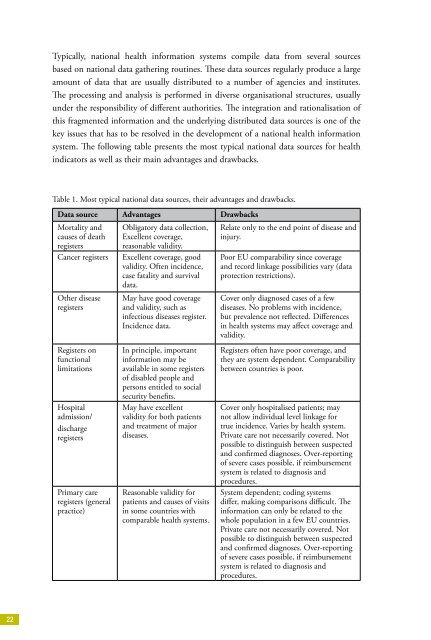
system. The following table presents the most typical national data sources for health<br />
indicators as well as their main advantages and drawbacks.<br />
Table 1. Most typical national data sources, their advantages and drawbacks.<br />
Data source Advantages Drawbacks<br />
Mortality and<br />
causes of death<br />
registers<br />
Cancer registers<br />
Other disease<br />
registers<br />
Registers on<br />
functional<br />
limitations<br />
Hospital<br />
admission/<br />
discharge<br />
registers<br />
Primary care<br />
registers (general<br />
practice)<br />
Obligatory data collection,<br />
Excellent coverage,<br />
reasonable validity.<br />
Excellent coverage, good<br />
validity. Often incidence,<br />
case fatality and survival<br />
data.<br />
May have good coverage<br />
and validity, such as<br />
infectious diseases register.<br />
Incidence data.<br />
In principle, important<br />
information may be<br />
available in some registers<br />
of disabled people and<br />
persons entitled to social<br />
security benefits.<br />
May have excellent<br />
validity for both patients<br />
and treatment of major<br />
diseases.<br />
Reasonable validity for<br />
patients and causes of visits<br />
in some countries with<br />
comparable health systems.<br />
Relate only to the end point of disease and<br />
injury.<br />
Poor EU comparability since coverage<br />
and record linkage possibilities vary (data<br />
protection restrictions).<br />
Cover only diagnosed cases of a few<br />
diseases. No problems with incidence,<br />
but prevalence not reflected. Differences<br />
in health systems may affect coverage and<br />
validity.<br />
Registers often have poor coverage, and<br />
they are system dependent. Comparability<br />
between countries is poor.<br />
Cover only hospitalised patients; may<br />
not allow individual level linkage for<br />
true incidence. Varies by health system.<br />
Private care not necessarily covered. Not<br />
possible to distinguish between suspected<br />
and confirmed diagnoses. Over-reporting<br />
of severe cases possible, if reimbursement<br />
system is related to diagnosis and<br />
procedures.<br />
System dependent; coding systems<br />
differ, making comparisons difficult. The<br />
information can only be related to the<br />
whole population in a few EU countries.<br />
Private care not necessarily covered. Not<br />
possible to distinguish between suspected<br />
and confirmed diagnoses. Over-reporting<br />
of severe cases possible, if reimbursement<br />
system is related to diagnosis and<br />
procedures.<br />
22