Dental Asia May/June 2018
For more than two decades, Dental Asia is the premium journal in linking dental innovators and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.
For more than two decades, Dental Asia is the premium journal in linking dental innovators
and manufacturers to its rightful audience. We devote ourselves in showcasing the latest dental technology and share evidence-based clinical philosophies to serve as an educational platform to dental professionals. Our combined portfolio of print and digital media also allows us to reach a wider market and secure our position as the leading dental media in the Asia Pacific region while facilitating global interactions among our readers.
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Clinical Feature<br />
In severe instances, the frenum may be attached high on the<br />
alveolar ridge, even into the region of the incisive papillae. When a<br />
lip-tie restricts the movement of the upper lip, it may be dicult for<br />
an infant to evert its upper lip and latch properly onto the breast.<br />
If the infant can only take the mother’s nipple into its mouth,<br />
rather than the surrounding areola, traumatic breakdown of the<br />
nipple may occur, causing pain and discomfort for the mother and<br />
an inadequate transfer of milk for the infant. 24 In 2004, Kotlow<br />
proposed a classication for lip-ties, this is displayed in Table 1. 25<br />
Tongue-tie, also known as ankyloglossia, is an abnormal lingual<br />
frenum which limits the normal range of movement and function<br />
of the tongue (Fig. 2). There is currently no consensus on a precise<br />
denition of ankyloglossia; however, several attempts have been<br />
made to categorise various types of tongue-tie based on both<br />
anatomy and functional limitations. Kotlow developed one of<br />
the most commonly used classications of tongue-tie (Table 2),<br />
based on the measurements of 322 children ranging from ages 18<br />
months to 14 years. 26 Class I and II tongue-tie is considered to be an<br />
anterior tongue-tie, while Class III and IV are referred to as posterior<br />
tongue-tie. 27 This dierentiation between anterior and posterior<br />
t o n g u e - t i e i s a r e l a t i v e l y a n e w d i s t i n c t i o n . U n l i k e a n t e r i o r<br />
tongue-tie, posterior tongue-tie is not obvious at rst glance as<br />
the frenum is hidden beneath the mucosal layer. There may not<br />
be a frenal membrane present, instead the diagnosis may be made<br />
based on the mid-tongue’s inability to elevate.<br />
Type Characteristics Range of tongue<br />
movement<br />
Clinically<br />
acceptable<br />
Table 2. Kotlow’s classication of the<br />
dierent types of ankyloglossia. 26<br />
Normal range of free<br />
tongue movements<br />
Greater than 16mm<br />
Class I Mild tongue-tie 12-16mm<br />
Class II Moderate tongue-tie 8-11mm<br />
Class III Severe tongue-tie 3-7mm<br />
Class IV Complete tongue-tie Less than 3mm<br />
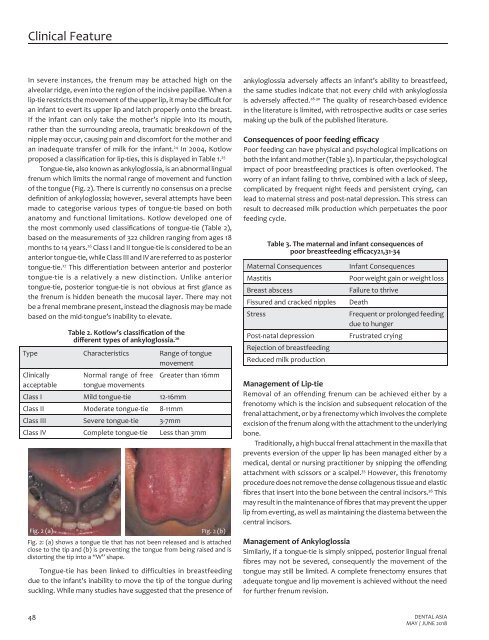
Fig. 2 (a)<br />
Fig. 2 (b)<br />
Fig. 2: (a) shows a tongue tie that has not been released and is attached<br />
close to the tip and (b) is preventing the tongue from being raised and is<br />
distorting the tip into a “W” shape.<br />
Tongue-tie has been linked to difficulties in breastfeeding<br />
due to the infant’s inability to move the tip of the tongue during<br />
suckling. While many studies have suggested that the presence of<br />
ankyloglossia adversely aects an infant’s ability to breastfeed,<br />
the same studies indicate that not every child with ankyloglossia<br />
is adversely aected. 28-30 The quality of research-based evidence<br />
in the literature is limited, with retrospective audits or case series<br />
making up the bulk of the published literature.<br />
Consequences of poor feeding ecacy<br />
Poor feeding can have physical and psychological implications on<br />
both the infant and mother (Table 3). In particular, the psychological<br />
impact of poor breastfeeding practices is often overlooked. The<br />
worry of an infant failing to thrive, combined with a lack of sleep,<br />
complicated by frequent night feeds and persistent crying, can<br />
lead to maternal stress and post-natal depression. This stress can<br />
result to decreased milk production which perpetuates the poor<br />
feeding cycle.<br />
Table 3. The maternal and infant consequences of<br />
poor breastfeeding ecacy21,31-34<br />
Maternal Consequences<br />
Mastitis<br />
Breast abscess<br />
Fissured and cracked nipples<br />
Stress<br />
Post-natal depression<br />
Rejection of breastfeeding<br />
Reduced milk production<br />
Infant Consequences<br />
Poor weight gain or weight loss<br />
Failure to thrive<br />
Death<br />
Frequent or prolonged feeding<br />
due to hunger<br />
Frustrated crying<br />
Management of Lip-tie<br />
Removal of an offending frenum can be achieved either by a<br />
frenotomy which is the incision and subsequent relocation of the<br />
frenal attachment, or by a frenectomy which involves the complete<br />
excision of the frenum along with the attachment to the underlying<br />
bone.<br />
Traditionally, a high buccal frenal attachment in the maxilla that<br />
prevents eversion of the upper lip has been managed either by a<br />
medical, dental or nursing practitioner by snipping the oending<br />
attachment with scissors or a scalpel. 35 However, this frenotomy<br />
procedure does not remove the dense collagenous tissue and elastic<br />
bres that insert into the bone between the central incisors. 36 This<br />
may result in the maintenance of bres that may prevent the upper<br />
lip from everting, as well as maintaining the diastema between the<br />
central incisors.<br />
Management of Ankyloglossia<br />
Similarly, if a tongue-tie is simply snipped, posterior lingual frenal<br />
bres may not be severed, consequently the movement of the<br />
tongue may still be limited. A complete frenectomy ensures that<br />
adequate tongue and lip movement is achieved without the need<br />
for further frenum revision.<br />
48 DENTAL ASIA<br />
MAY / JUNE <strong>2018</strong>