

Report in English with a Dutch summary (KCE reports 63A)
Report in English with a Dutch summary (KCE reports 63A)
Report in English with a Dutch summary (KCE reports 63A)

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
132 Breast Cancer <strong>KCE</strong> <strong>reports</strong> 63<br />
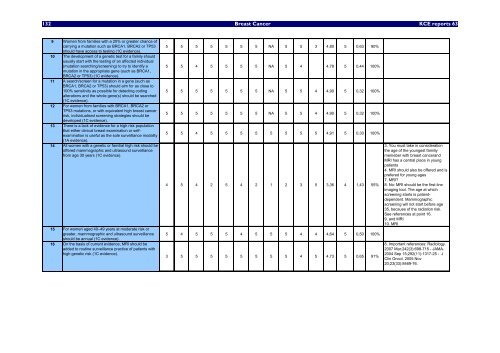
9 Women from families <strong>with</strong> a 20% or greater chance of<br />
carry<strong>in</strong>g a mutation such as BRCA1, BRCA2 or TP53<br />
should have access to test<strong>in</strong>g (1C evidence).<br />
10 The development of a genetic test for a family should<br />
usually start <strong>with</strong> the test<strong>in</strong>g of an affected <strong>in</strong>dividual<br />
(mutation search<strong>in</strong>g/screen<strong>in</strong>g) to try to identify a<br />
mutation <strong>in</strong> the appropriate gene (such as BRCA1,<br />
BRCA2 or TP53) (1C evidence).<br />
11 A search/screen for a mutation <strong>in</strong> a gene (such as<br />
BRCA1, BRCA2 or TP53) should aim for as close to<br />
100% sensitivity as possible for detect<strong>in</strong>g cod<strong>in</strong>g<br />
alterations and the whole gene(s) should be searched<br />
(1C evidence).<br />
12 For women from families <strong>with</strong> BRCA1, BRCA2 or<br />
TP53 mutations, or <strong>with</strong> equivalent high breast cancer<br />
risk, <strong>in</strong>dividualised screen<strong>in</strong>g strategies should be<br />
developed (1C evidence).<br />
13 There is a lack of evidence for a high risk population<br />
that either cl<strong>in</strong>ical breast exam<strong>in</strong>ation or selfexam<strong>in</strong>ation<br />
is useful as the sole surveillance modality<br />
(1A evidence).<br />
14 All women <strong>with</strong> a genetic or familial high risk should be<br />
offered mammographic and ultrasound surveillance<br />
from age 30 years (1C evidence).<br />
15 For women aged 40–49 years at moderate risk or<br />
greater, mammographic and ultrasound surveillance<br />
should be annual (1C evidence).<br />
16 On the basis of current evidence, MRI should be<br />
added to rout<strong>in</strong>e surveillance practice of patients <strong>with</strong><br />
high genetic risk (1C evidence).<br />
5 5 5 5 5 5 5 NA 5 5 3 4,80 5 0,63 90%<br />
5 5 4 5 5 5 5 NA 5 4 4,78 5 0,44 100%<br />
5 5 5 5 5 5 5 NA 5 5 4 4,90 5 0,32 100%<br />
5 5 5 5 5 5 5 NA 5 5 4 4,90 5 0,32 100%<br />
5 5 4 5 5 5 5 5 5 5 5 4,91 5 0,30 100%<br />
4 5 4 2 5 4 2 1 2 3 5 3,36 4 1,43 55%<br />
5 4 5 5 5 4 5 5 5 4 4 4,64 5 0,50 100%<br />
3 5 5 5 5 5 5 5 5 4 5 4,73 5 0,65 91%<br />
3. You must take <strong>in</strong> consideration<br />
the age of the youngest familiy<br />
memeber <strong>with</strong> breast cancerand<br />
MRI has a central place <strong>in</strong> young<br />
patients<br />
4. MRI should also be offered and is<br />
prefered for young ages<br />
7. MRI?<br />
8. No: MRI should be the first-l<strong>in</strong>e<br />
imag<strong>in</strong>g tool. The age at which<br />
screen<strong>in</strong>g starts is patientdependent.<br />
Mammographic<br />
screen<strong>in</strong>g will not start before age<br />
35, because of the radiation risk.<br />
See references at po<strong>in</strong>t 16.<br />
9. and MRI<br />
10. MRI<br />
8. Important references: Radiology.<br />
2007 Mar;242(3):698-715 - JAMA.<br />
2004 Sep 15;292(11):1317-25 - J<br />
Cl<strong>in</strong> Oncol. 2005 Nov<br />
20;23(33):8469-76.













