

Congenital malformations - Edocr
Congenital malformations - Edocr
Congenital malformations - Edocr

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
228 PART VI GASTROINTESTINAL MALFORMATIONS<br />
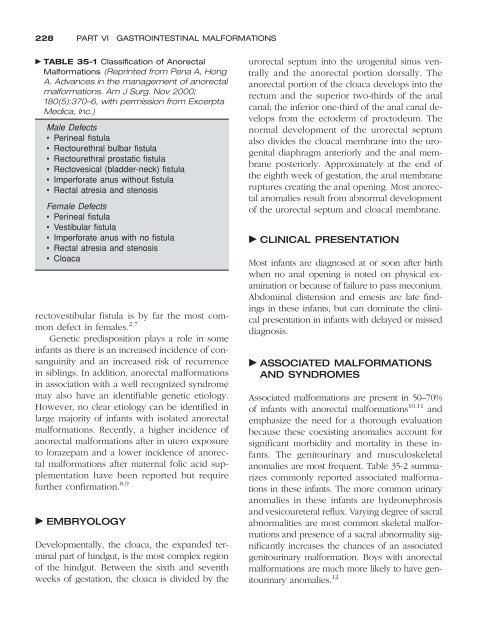
TABLE 35-1 Classification of Anorectal<br />
Malformations (Reprinted from Pena A, Hong<br />
A. Advances in the management of anorectal<br />
<strong>malformations</strong>. Am J Surg. Nov 2000;<br />
180(5):370–6, with permission from Excerpta<br />
Medica, Inc.)<br />
Male Defects<br />
• Perineal fistula<br />
• Rectourethral bulbar fistula<br />
• Rectourethral prostatic fistula<br />
• Rectovesical (bladder-neck) fistula<br />
• Imperforate anus without fistula<br />
• Rectal atresia and stenosis<br />
Female Defects<br />
• Perineal fistula<br />
• Vestibular fistula<br />
• Imperforate anus with no fistula<br />
• Rectal atresia and stenosis<br />
• Cloaca<br />
rectovestibular fistula is by far the most common<br />
defect in females. 2,7<br />
Genetic predisposition plays a role in some<br />
infants as there is an increased incidence of consanguinity<br />
and an increased risk of recurrence<br />
in siblings. In addition, anorectal <strong>malformations</strong><br />
in association with a well recognized syndrome<br />
may also have an identifiable genetic etiology.<br />
However, no clear etiology can be identified in<br />
large majority of infants with isolated anorectal<br />
<strong>malformations</strong>. Recently, a higher incidence of<br />
anorectal <strong>malformations</strong> after in utero exposure<br />
to lorazepam and a lower incidence of anorectal<br />
<strong>malformations</strong> after maternal folic acid supplementation<br />
have been reported but require<br />
further confirmation. 8,9<br />
EMBRYOLOGY<br />
Developmentally, the cloaca, the expanded terminal<br />
part of hindgut, is the most complex region<br />
of the hindgut. Between the sixth and seventh<br />
weeks of gestation, the cloaca is divided by the<br />
urorectal septum into the urogenital sinus ventrally<br />
and the anorectal portion dorsally. The<br />
anorectal portion of the cloaca develops into the<br />
rectum and the superior two-thirds of the anal<br />
canal; the inferior one-third of the anal canal develops<br />
from the ectoderm of proctodeum. The<br />
normal development of the urorectal septum<br />
also divides the cloacal membrane into the urogenital<br />
diaphragm anteriorly and the anal membrane<br />
posteriorly. Approximately at the end of<br />
the eighth week of gestation, the anal membrane<br />
ruptures creating the anal opening. Most anorectal<br />
anomalies result from abnormal development<br />
of the urorectal septum and cloacal membrane.<br />
CLINICAL PRESENTATION<br />
Most infants are diagnosed at or soon after birth<br />
when no anal opening is noted on physical examination<br />
or because of failure to pass meconium.<br />
Abdominal distension and emesis are late findings<br />
in these infants, but can dominate the clinical<br />
presentation in infants with delayed or missed<br />
diagnosis.<br />
ASSOCIATED MALFORMATIONS<br />
AND SYNDROMES<br />
Associated <strong>malformations</strong> are present in 50–70%<br />
of infants with anorectal <strong>malformations</strong> 10,11 and<br />
emphasize the need for a thorough evaluation<br />
because these coexisting anomalies account for<br />
significant morbidity and mortality in these infants.<br />
The genitourinary and musculoskeletal<br />
anomalies are most frequent. Table 35-2 summarizes<br />
commonly reported associated <strong>malformations</strong><br />
in these infants. The more common urinary<br />
anomalies in these infants are hydronephrosis<br />
and vesicoureteral reflux. Varying degree of sacral<br />
abnormalities are most common skeletal <strong>malformations</strong><br />
and presence of a sacral abnormality significantly<br />
increases the chances of an associated<br />
genitourinary malformation. Boys with anorectal<br />
<strong>malformations</strong> are much more likely to have genitourinary<br />
anomalies. 12













