

Congenital malformations - Edocr
Congenital malformations - Edocr
Congenital malformations - Edocr

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
CHAPTER 36 HIRSCHSPRUNG DISEASE 237<br />
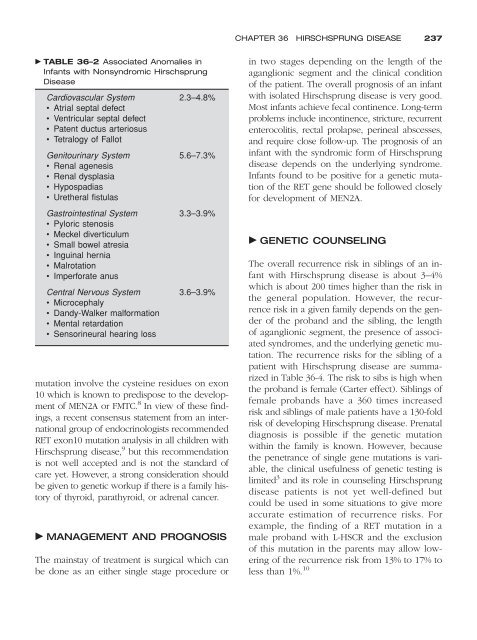
TABLE 36–2 Associated Anomalies in<br />
Infants with Nonsyndromic Hirschsprung<br />
Disease<br />
Cardiovascular System 2.3–4.8%<br />
• Atrial septal defect<br />
• Ventricular septal defect<br />
• Patent ductus arteriosus<br />
• Tetralogy of Fallot<br />
Genitourinary System 5.6–7.3%<br />
• Renal agenesis<br />
• Renal dysplasia<br />
• Hypospadias<br />
• Uretheral fistulas<br />
Gastrointestinal System 3.3–3.9%<br />
• Pyloric stenosis<br />
• Meckel diverticulum<br />
• Small bowel atresia<br />
• Inguinal hernia<br />
• Malrotation<br />
• Imperforate anus<br />
Central Nervous System 3.6–3.9%<br />
• Microcephaly<br />
• Dandy-Walker malformation<br />
• Mental retardation<br />
• Sensorineural hearing loss<br />
mutation involve the cysteine residues on exon<br />
10 which is known to predispose to the development<br />
of MEN2A or FMTC. 8 In view of these findings,<br />
a recent consensus statement from an international<br />
group of endocrinologists recommended<br />
RET exon10 mutation analysis in all children with<br />
Hirschsprung disease, 9 but this recommendation<br />
is not well accepted and is not the standard of<br />
care yet. However, a strong consideration should<br />
be given to genetic workup if there is a family history<br />
of thyroid, parathyroid, or adrenal cancer.<br />
MANAGEMENT AND PROGNOSIS<br />
The mainstay of treatment is surgical which can<br />
be done as an either single stage procedure or<br />
in two stages depending on the length of the<br />
aganglionic segment and the clinical condition<br />
of the patient. The overall prognosis of an infant<br />
with isolated Hirschsprung disease is very good.<br />
Most infants achieve fecal continence. Long-term<br />
problems include incontinence, stricture, recurrent<br />
enterocolitis, rectal prolapse, perineal abscesses,<br />
and require close follow-up. The prognosis of an<br />
infant with the syndromic form of Hirschsprung<br />
disease depends on the underlying syndrome.<br />
Infants found to be positive for a genetic mutation<br />
of the RET gene should be followed closely<br />
for development of MEN2A.<br />
GENETIC COUNSELING<br />
The overall recurrence risk in siblings of an infant<br />
with Hirschsprung disease is about 3–4%<br />
which is about 200 times higher than the risk in<br />
the general population. However, the recurrence<br />
risk in a given family depends on the gender<br />
of the proband and the sibling, the length<br />
of aganglionic segment, the presence of associated<br />
syndromes, and the underlying genetic mutation.<br />
The recurrence risks for the sibling of a<br />
patient with Hirschsprung disease are summarized<br />
in Table 36-4. The risk to sibs is high when<br />
the proband is female (Carter effect). Siblings of<br />
female probands have a 360 times increased<br />
risk and siblings of male patients have a 130-fold<br />
risk of developing Hirschsprung disease. Prenatal<br />
diagnosis is possible if the genetic mutation<br />
within the family is known. However, because<br />
the penetrance of single gene mutations is variable,<br />
the clinical usefulness of genetic testing is<br />
limited 3 and its role in counseling Hirschsprung<br />
disease patients is not yet well-defined but<br />
could be used in some situations to give more<br />
accurate estimation of recurrence risks. For<br />
example, the finding of a RET mutation in a<br />
male proband with L-HSCR and the exclusion<br />
of this mutation in the parents may allow lowering<br />
of the recurrence risk from 13% to 17% to<br />
less than 1%. 10













