

Guidelines for a Palliative Approach in Residential Aged Care
Guidelines for a Palliative Approach in Residential Aged Care
Guidelines for a Palliative Approach in Residential Aged Care

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
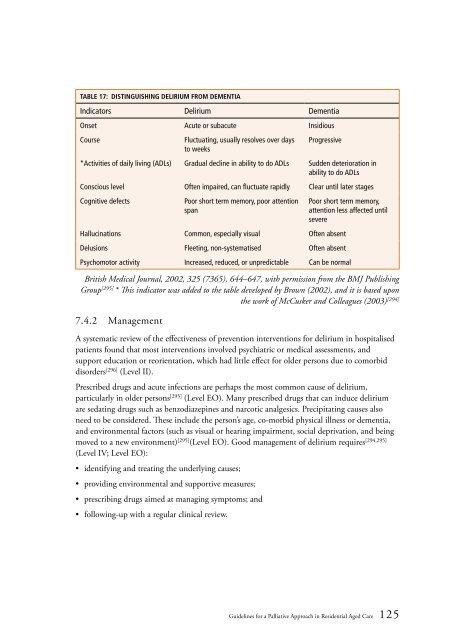
Table 17: Dist<strong>in</strong>guish<strong>in</strong>g delirium from dementia<br />
Indicators Delirium Dementia<br />
Onset Acute or subacute Insidious<br />
Course<br />
Fluctuat<strong>in</strong>g, usually resolves over days<br />
to weeks<br />
Progressive<br />
*Activities of daily liv<strong>in</strong>g (ADLs) Gradual decl<strong>in</strong>e <strong>in</strong> ability to do ADLs Sudden deterioration <strong>in</strong><br />
ability to do ADLs<br />
Conscious level Often impaired, can fluctuate rapidly Clear until later stages<br />
Cognitive defects<br />
Poor short term memory, poor attention<br />
span<br />
Halluc<strong>in</strong>ations Common, especially visual Often absent<br />
Delusions Fleet<strong>in</strong>g, non-systematised Often absent<br />
Poor short term memory,<br />
attention less affected until<br />
severe<br />
Psychomotor activity Increased, reduced, or unpredictable Can be normal<br />
British Medical Journal, 2002, 325 (7365), 644–647, with permission from the BMJ Publish<strong>in</strong>g<br />
Group [295] * This <strong>in</strong>dicator was added to the table developed by Brown (2002), and it is based upon<br />
the work of McCusker and Colleagues (2003) [294]<br />
7.4.2 Management<br />
A systematic review of the effectiveness of prevention <strong>in</strong>terventions <strong>for</strong> delirium <strong>in</strong> hospitalised<br />
patients found that most <strong>in</strong>terventions <strong>in</strong>volved psychiatric or medical assessments, and<br />
support education or reorientation, which had little effect <strong>for</strong> older persons due to comorbid<br />
disorders [296] (Level II).<br />
Prescribed drugs and acute <strong>in</strong>fections are perhaps the most common cause of delirium,<br />
particularly <strong>in</strong> older persons [295] (Level EO). Many prescribed drugs that can <strong>in</strong>duce delirium<br />
are sedat<strong>in</strong>g drugs such as benzodiazep<strong>in</strong>es and narcotic analgesics. Precipitat<strong>in</strong>g causes also<br />
need to be considered. These <strong>in</strong>clude the person’s age, co-morbid physical illness or dementia,<br />
and environmental factors (such as visual or hear<strong>in</strong>g impairment, social deprivation, and be<strong>in</strong>g<br />
moved to a new environment) [295] (Level EO). Good management of delirium requires [294,295]<br />
(Level IV; Level EO):<br />
• identify<strong>in</strong>g and treat<strong>in</strong>g the underly<strong>in</strong>g causes;<br />
• provid<strong>in</strong>g environmental and supportive measures;<br />
• prescrib<strong>in</strong>g drugs aimed at manag<strong>in</strong>g symptoms; and<br />
• follow<strong>in</strong>g-up with a regular cl<strong>in</strong>ical review.<br />
<strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> a <strong>Palliative</strong> <strong>Approach</strong> <strong>in</strong> <strong>Residential</strong> <strong>Aged</strong> <strong>Care</strong> 125













