

Guidelines for a Palliative Approach in Residential Aged Care
Guidelines for a Palliative Approach in Residential Aged Care
Guidelines for a Palliative Approach in Residential Aged Care

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
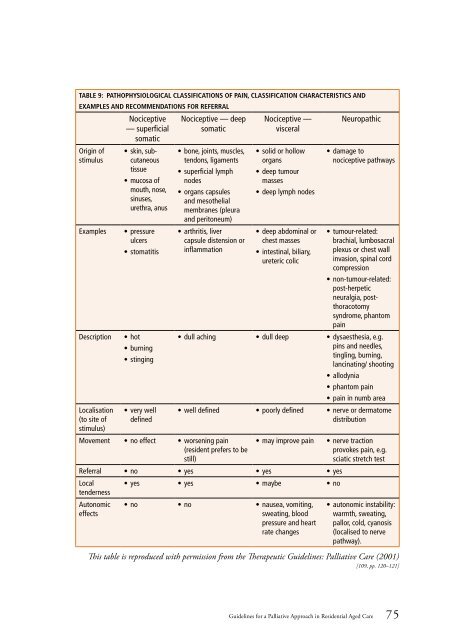
Table 9: Pathophysiological classifications of pa<strong>in</strong>, classification characteristics and<br />
examples and recommendations <strong>for</strong> referral<br />
Orig<strong>in</strong> of<br />
stimulus<br />
Examples<br />
Description<br />
Localisation<br />
(to site of<br />
stimulus)<br />
Nociceptive<br />
— superficial<br />
somatic<br />
• sk<strong>in</strong>, subcutaneous<br />
tissue<br />
• mucosa of<br />
mouth, nose,<br />
s<strong>in</strong>uses,<br />
urethra, anus<br />
• pressure<br />
ulcers<br />
• stomatitis<br />
• hot<br />
• burn<strong>in</strong>g<br />
• st<strong>in</strong>g<strong>in</strong>g<br />
• very well<br />
def<strong>in</strong>ed<br />
Nociceptive — deep<br />
somatic<br />
• bone, jo<strong>in</strong>ts, muscles,<br />
tendons, ligaments<br />
• superficial lymph<br />
nodes<br />
• organs capsules<br />
and mesothelial<br />
membranes (pleura<br />
and peritoneum)<br />
• arthritis, liver<br />
capsule distension or<br />
<strong>in</strong>flammation<br />
Movement • no effect • worsen<strong>in</strong>g pa<strong>in</strong><br />
(resident prefers to be<br />
still)<br />
Nociceptive —<br />
visceral<br />
• solid or hollow<br />
organs<br />
• deep tumour<br />
masses<br />
• deep lymph nodes<br />
• deep abdom<strong>in</strong>al or<br />
chest masses<br />
• <strong>in</strong>test<strong>in</strong>al, biliary,<br />
ureteric colic<br />
Neuropathic<br />
• damage to<br />
nociceptive pathways<br />
• tumour-related:<br />
brachial, lumbosacral<br />
plexus or chest wall<br />
<strong>in</strong>vasion, sp<strong>in</strong>al cord<br />
compression<br />
• non-tumour-related:<br />
post-herpetic<br />
neuralgia, postthoracotomy<br />
syndrome, phantom<br />
pa<strong>in</strong><br />
• dull ach<strong>in</strong>g • dull deep • dysaesthesia, e.g.<br />
p<strong>in</strong>s and needles,<br />
t<strong>in</strong>gl<strong>in</strong>g, burn<strong>in</strong>g,<br />
lanc<strong>in</strong>at<strong>in</strong>g/ shoot<strong>in</strong>g<br />
• allodynia<br />
• phantom pa<strong>in</strong><br />
• pa<strong>in</strong> <strong>in</strong> numb area<br />
• well def<strong>in</strong>ed • poorly def<strong>in</strong>ed • nerve or dermatome<br />
distribution<br />
• may improve pa<strong>in</strong><br />
Referral • no • yes • yes • yes<br />
Local<br />
tenderness<br />
Autonomic<br />
effects<br />
• yes • yes • maybe • no<br />
• no • no • nausea, vomit<strong>in</strong>g,<br />
sweat<strong>in</strong>g, blood<br />
pressure and heart<br />
rate changes<br />
• nerve traction<br />
provokes pa<strong>in</strong>, e.g.<br />
sciatic stretch test<br />
• autonomic <strong>in</strong>stability:<br />
warmth, sweat<strong>in</strong>g,<br />
pallor, cold, cyanosis<br />
(localised to nerve<br />
pathway).<br />
This table is reproduced with permission from the Therapeutic <strong>Guidel<strong>in</strong>es</strong>: <strong>Palliative</strong> <strong>Care</strong> (2001)<br />
[109, pp. 120–121]<br />
<strong>Guidel<strong>in</strong>es</strong> <strong>for</strong> a <strong>Palliative</strong> <strong>Approach</strong> <strong>in</strong> <strong>Residential</strong> <strong>Aged</strong> <strong>Care</strong> 75













