

2,46 Mb - GuÃaSalud
2,46 Mb - GuÃaSalud
2,46 Mb - GuÃaSalud

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
C<br />
B<br />
D<br />
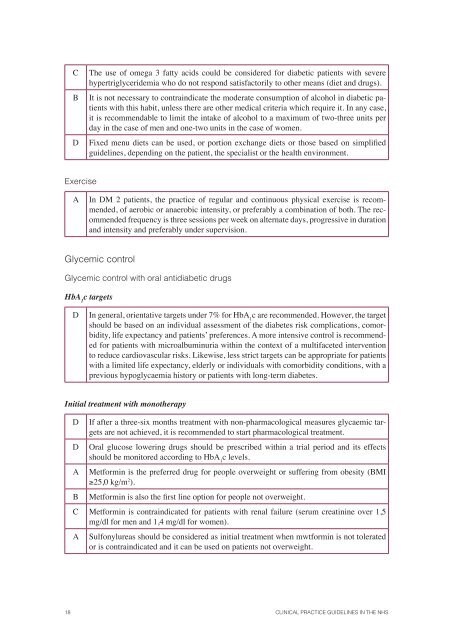
The use of omega 3 fatty acids could be considered for diabetic patients with severe<br />
hypertriglyceridemia who do not respond satisfactorily to other means (diet and drugs).<br />
It is not necessary to contraindicate the moderate consumption of alcohol in diabetic patients<br />
with this habit, unless there are other medical criteria which require it. In any case,<br />
it is recommendable to limit the intake of alcohol to a maximum of two-three units per<br />
day in the case of men and one-two units in the case of women.<br />
Fixed menu diets can be used, or portion exchange diets or those based on simplified<br />
guidelines, depending on the patient, the specialist or the health environment.<br />
Exercise<br />
A<br />
In DM 2 patients, the practice of regular and continuous physical exercise is recommended,<br />
of aerobic or anaerobic intensity, or preferably a combination of both. The recommended<br />
frequency is three sessions per week on alternate days, progressive in duration<br />
and intensity and preferably under supervision.<br />
Glycemic control<br />
Glycemic control with oral antidiabetic drugs<br />
HbA 1<br />
c targets<br />
D<br />
In general, orientative targets under 7% for HbA 1<br />
c are recommended. However, the target<br />
should be based on an individual assessment of the diabetes risk complications, comorbidity,<br />
life expectancy and patients’ preferences. A more intensive control is recommended<br />
for patients with microalbuminuria within the context of a multifaceted intervention<br />
to reduce cardiovascular risks. Likewise, less strict targets can be appropriate for patients<br />
with a limited life expectancy, elderly or individuals with comorbidity conditions, with a<br />
previous hypoglycaemia history or patients with long-term diabetes.<br />
Initial treatment with monotherapy<br />
D<br />
D<br />
A<br />
B<br />
If after a three-six months treatment with non-pharmacological measures glycaemic targets<br />
are not achieved, it is recommended to start pharmacological treatment.<br />
Oral glucose lowering drugs should be prescribed within a trial period and its effects<br />
should be monitored according to HbA 1<br />
c levels.<br />
Metformin is the preferred drug for people overweight or suffering from obesity (BMI<br />
≥25,0 kg/m 2 ).<br />
Metformin is also the first line option for people not overweight.<br />
C Metformin is contraindicated for patients with renal failure (serum creatinine over 1,5<br />
mg/dl for men and 1,4 mg/dl for women).<br />
A<br />
Sulfonylureas should be considered as initial treatment when mwtformin is not tolerated<br />
or is contraindicated and it can be used on patients not overweight.<br />
18 CLINICAL PRACTICE GUIDELINES IN THE NHS














