

Vol 44 # 4 December 2012 - Kma.org.kw
Vol 44 # 4 December 2012 - Kma.org.kw
Vol 44 # 4 December 2012 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>December</strong> <strong>2012</strong><br />
KUWAIT MEDICAL JOURNAL 330<br />
Fig. 1: Laparoscopic photograph showing the base of double<br />
appendix (arrows) and attached mesoappendix in-between<br />
Fig. 3: Photomicrograph showing the two separate mucosas (arrows)<br />
of the double appendix with two separate muscle coats and both<br />
muscular walls separated by meso-appendicular fibroadipose tissue<br />
( H & E stain X20)<br />
of small and large bowels, which ruled out any other<br />
associated congenital anomaly. Her postoperative<br />
course was uneventful and she was discharged on<br />
postoperative day five.<br />
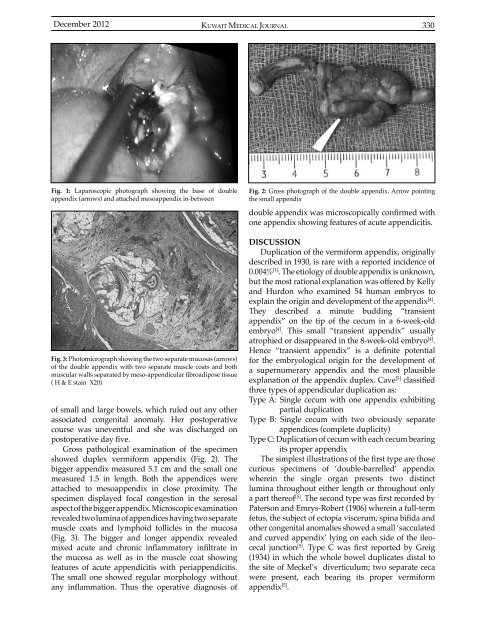
Gross pathological examination of the specimen<br />
showed duplex vermiform appendix (Fig. 2). The<br />
bigger appendix measured 5.1 cm and the small one<br />
measured 1.5 in length. Both the appendices were<br />
attached to mesoappendix in close proximity. The<br />
specimen displayed focal congestion in the serosal<br />
aspect of the bigger appendix. Microscopic examination<br />
revealed two lumina of appendices having two separate<br />
muscle coats and lymphoid follicles in the mucosa<br />
(Fig. 3). The bigger and longer appendix revealed<br />
mixed acute and chronic inflammatory infiltrate in<br />
the mucosa as well as in the muscle coat showing<br />
features of acute appendicitis with periappendicitis.<br />
The small one showed regular morphology without<br />
any inflammation. Thus the operative diagnosis of<br />
Fig. 2: Gross photograph of the double appendix. Arrow pointing<br />
the small appendix<br />
double appendix was microscopically confirmed with<br />
one appendix showing features of acute appendicitis.<br />
DISCUSSION<br />
Duplication of the vermiform appendix, originally<br />
described in 1930, is rare with a reported incidence of<br />
0.004% [1] . The etiology of double appendix is unknown,<br />
but the most rational explanation was offered by Kelly<br />
and Hurdon who examined 54 human embryos to<br />
explain the origin and development of the appendix [4] .<br />
They described a minute budding “transient<br />
appendix” on the tip of the cecum in a 6-week-old<br />
embryo [4] . This small “transient appendix” usually<br />
atrophied or disappeared in the 8-week-old embryo [4] .<br />
Hence “transient appendix” is a definite potential<br />
for the embryological origin for the development of<br />
a supernumerary appendix and the most plausible<br />
explanation of the appendix duplex. Cave [5] classified<br />
three types of appendicular duplication as:<br />
Type A: Single cecum with one appendix exhibiting<br />
partial duplication<br />
Type B: Single cecum with two obviously separate<br />
appendices (complete duplicity)<br />
Type C: Duplication of cecum with each cecum bearing<br />
its proper appendix<br />
The simplest illustrations of the first type are those<br />
curious specimens of ‘double-barrelled’ appendix<br />
wherein the single <strong>org</strong>an presents two distinct<br />
lumina throughout either length or throughout only<br />
a part thereof [5] . The second type was first recorded by<br />
Paterson and Emrys-Robert (1906) wherein a full-term<br />
fetus, the subject of ectopia viscerum, spina bifida and<br />
other congenital anomalies showed a small ‘sacculated<br />
and curved appendix’ lying on each side of the ileocecal<br />
junction [5] . Type C was first reported by Greig<br />
(1934) in which the whole bowel duplicates distal to<br />
the site of Meckel’s diverticulum; two separate ceca<br />
were present, each bearing its proper vermiform<br />
appendix [5] .













