PARKLAND HEALTHfirst - Parkland Community Health Plan, Inc.
PARKLAND HEALTHfirst - Parkland Community Health Plan, Inc.
PARKLAND HEALTHfirst - Parkland Community Health Plan, Inc.

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
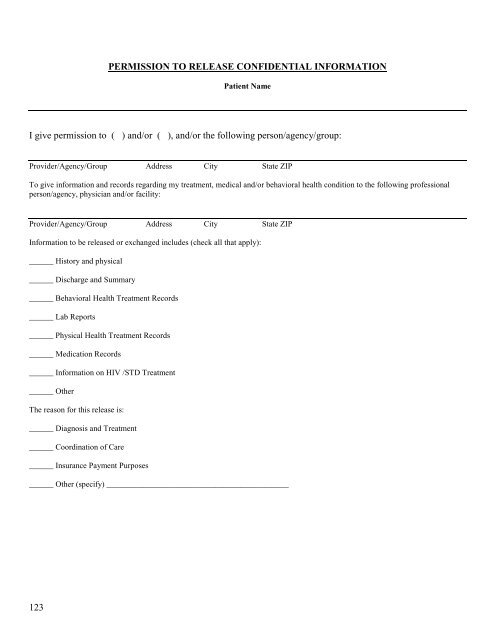
PERMISSION TO RELEASE CONFIDENTIAL INFORMATION<br />
Patient Name<br />
I give permission to ( ) and/or ( ), and/or the following person/agency/group:<br />
Provider/Agency/Group Address City State ZIP<br />
To give information and records regarding my treatment, medical and/or behavioral health condition to the following professional<br />
person/agency, physician and/or facility:<br />
Provider/Agency/Group Address City State ZIP<br />
Information to be released or exchanged includes (check all that apply):<br />
______ History and physical<br />
______ Discharge and Summary<br />
______ Behavioral <strong>Health</strong> Treatment Records<br />
______ Lab Reports<br />
______ Physical <strong>Health</strong> Treatment Records<br />
______ Medication Records<br />
______ Information on HIV /STD Treatment<br />
______ Other<br />
The reason for this release is:<br />
______ Diagnosis and Treatment<br />
______ Coordination of Care<br />
______ Insurance Payment Purposes<br />
______ Other (specify) _____________________________________________<br />
123