Latvia
Latvia
Latvia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Health systems in transition<br />
<strong>Latvia</strong><br />
earmarked portion of centrally collected income tax (28.4% of personal income<br />
tax revenue) plus a state subsidy financed by general tax revenue.<br />
A process of further “recentralization” was initiated at the end of the decade<br />
and ended in 2004. As part of this process, the eight regional sickness funds were<br />
merged into one single central state agency, the SCHIA, with its five territorial<br />
branches and unified allocation, payment and control mechanisms. The health<br />
care funds were allocated from the central government budget (much like a taxfinanced<br />
health care system) to the SCHIA. Moreover, health budget funds that<br />
were previously allocated from the Ministry of Health directly to certain state<br />
agencies and health programmes began to be channelled through the SCHIA.<br />
In 2004, the earmarked payroll tax for health revenue base (28.4% of personal<br />
income tax revenues) was abandoned. The new system began operating in full<br />
in January 2005.<br />
The gradual centralization of financing was prompted by high levels of<br />
patient dissatisfaction, along with the perception among policy-makers that<br />
a decentralized system operating in <strong>Latvia</strong>’s relatively small territory and<br />
serving a small population gave rise to excessive inefficiencies in resource<br />
use and allocation. The need to save on public resources through more rational<br />
organization of financing was especially pronounced in view of serious funding<br />
shortfalls in health care relative to health care needs and demands, highlighting<br />
the need to address organizational weaknesses and failures and unnecessarily<br />
complicated payment methods.<br />
In 1997, the local health boards were disbanded. Not all local governments<br />
had a representative responsible for health. This has contributed to weakening<br />
the position of health in the local government agendas, and has had a negative<br />
impact particularly in the area of investment and infrastructure development,<br />
which could have been financed from municipal budgets.<br />
Other centralization tendencies<br />
Centralization tendencies are also evident at the service provider level. For<br />
instance, in the 1990s and at the start of the new millennium, hospital directors<br />
were free to make decisions on wage levels within their hospital. Very often,<br />
however, payments for the purchase of new technologies, or for infrastructure<br />
costs, were given priority over the payment of adequate salaries. Now, minimum<br />
salary levels according to specialties, position, seniority, etc. are established<br />
and regulated by the State.<br />
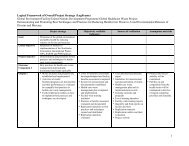
A special example of centralization is the “Master Plan for the development<br />
of outpatient and inpatient health care service providers”, involving planning at<br />
the central level for the entire country in order to rationalize the distribution of<br />
51