Smoking and mental health - NCSCT
Smoking and mental health - NCSCT
Smoking and mental health - NCSCT

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Smoking</strong> <strong>and</strong> <strong>mental</strong> <strong>health</strong><br />
research evidence has shown that implementation of smoke-free policies in<br />
<strong>mental</strong> <strong>health</strong>care settings is unlikely to result in deteriorations in <strong>mental</strong> state,<br />
or increased levels of aggression, violence, use of seclusion, discharge against<br />
medical advice or increased use of medication on an ‘as required’ basis. 7<br />
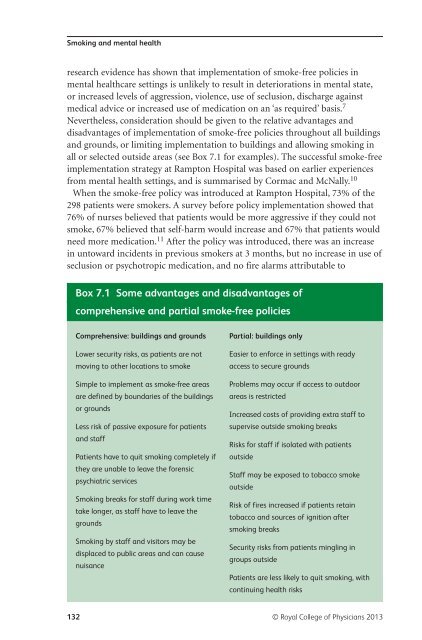
Nevertheless, consideration should be given to the relative advantages <strong>and</strong><br />
disadvantages of implementation of smoke-free policies throughout all buildings<br />
<strong>and</strong> grounds, or limiting implementation to buildings <strong>and</strong> allowing smoking in<br />
all or selected outside areas (see Box 7.1 for examples). The successful smoke-free<br />
implementation strategy at Rampton Hospital was based on earlier experiences<br />
from <strong>mental</strong> <strong>health</strong> settings, <strong>and</strong> is summarised by Cormac <strong>and</strong> McNally. 10<br />
When the smoke-free policy was introduced at Rampton Hospital, 73% of the<br />
298 patients were smokers. A survey before policy implementation showed that<br />
76% of nurses believed that patients would be more aggressive if they could not<br />
smoke, 67% believed that self-harm would increase <strong>and</strong> 67% that patients would<br />
need more medication. 11 After the policy was introduced, there was an increase<br />
in untoward incidents in previous smokers at 3 months, but no increase in use of<br />
seclusion or psychotropic medication, <strong>and</strong> no fire alarms attributable to<br />
Box 7.1 Some advantages <strong>and</strong> disadvantages of<br />
comprehensive <strong>and</strong> partial smoke-free policies<br />
Comprehensive: buildings <strong>and</strong> grounds<br />
Lower security risks, as patients are not<br />
moving to other locations to smoke<br />
Simple to implement as smoke-free areas<br />
are defined by boundaries of the buildings<br />
or grounds<br />
Less risk of passive exposure for patients<br />
<strong>and</strong> staff<br />
Patients have to quit smoking completely if<br />
they are unable to leave the forensic<br />
psychiatric services<br />
<strong>Smoking</strong> breaks for staff during work time<br />
take longer, as staff have to leave the<br />
grounds<br />
<strong>Smoking</strong> by staff <strong>and</strong> visitors may be<br />
displaced to public areas <strong>and</strong> can cause<br />
nuisance<br />
Partial: buildings only<br />
Easier to enforce in settings with ready<br />
access to secure grounds<br />
Problems may occur if access to outdoor<br />
areas is restricted<br />
Increased costs of providing extra staff to<br />
supervise outside smoking breaks<br />
Risks for staff if isolated with patients<br />
outside<br />
Staff may be exposed to tobacco smoke<br />
outside<br />
Risk of fires increased if patients retain<br />
tobacco <strong>and</strong> sources of ignition after<br />
smoking breaks<br />
Security risks from patients mingling in<br />
groups outside<br />
Patients are less likely to quit smoking, with<br />
continuing <strong>health</strong> risks<br />
132 © Royal College of Physicians 2013