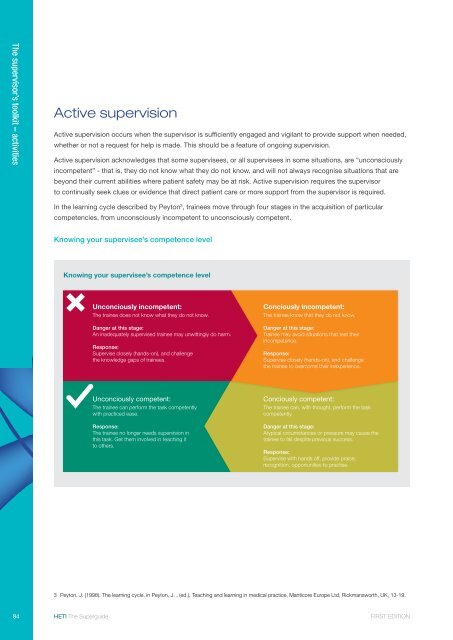
The supervisor’s toolkit – activitiesActive supervisionActive supervision occurs when the supervisor is sufficiently engaged and vigilant to provide support when needed,whether or not a request for help is made. This should be a feature of ongoing supervision.Active supervision acknowledges that some supervisees, or all supervisees in some situations, are “unconsciouslyincompetent” - that is, they do not know what they do not know, and will not always recognise situations that arebeyond their current abilities where patient safety may be at risk. Active supervision requires the supervisorto continually seek clues or evidence that direct patient care or more support from the supervisor is required.In the learning cycle described by Peyton 3 , trainees move through four stages in the acquisition of particularcompetencies, from unconsciously incompetent to unconsciously competent.Knowing your supervisee’s competence levelKnowing your supervisee’s competence levelUnconciously incompetent:The trainee does not know what they do not know.Danger at this stage:An inadequately supervised trainee may unwittingly do harm.Response:Supervise closely (hands-on), and challengethe knowledge gaps of trainees.Conciously incompetent:The trainee know that they do not know.Danger at this stage:Trainee may avoid situations that test theirincompetence.Response:Supervise closely (hands-on), and challengethe trainee to overcome their inexperience.Unconciously competent:The trainee can perform the task competentlywith practiced ease.Response:The trainee no longer needs supervision inthis task. Get them involved in teaching itto others.Conciously competent:The trainee can, with thought, perform the taskcompetently.Danger at this stage:Atypical circumstances or pressure may cause thetrainee to fail despite previous success.Response:Supervise with hands off, provide praise,recognition, opportunities to practise.3 Peyton, J. (1998). The learning cycle, in Peyton, J. , (ed.), Teaching and learning in medical practice, Manticore Europe Ltd, Rickmansworth, UK, 13-19.84 <strong>HETI</strong> The Superguide FIRST EDITION
A key concept: hands-on, hands-offAn effective supervisor knows when to give supervisees “Hands-on” supervisiondirection and when to give them freedom of action.• Guidance on interventions that requireTo move the supervisee from consciously incompetentfurther skills developmentto consciously competent, the supervisor must activelycalibrate the level of support provided.• Specific skills training sessionsThe supervisor’s toolkit – activitiesIedema et al. 4 put forward a model of clinical supervisionthat recognises the need for support and independence.It was found that supervisees value supervisory supportof two kinds:“Hands-on” supervision — when the supervisor isdirectly involved in monitoring or helping the superviseeas he/she performs tasks.“Hands-off” supervision — when the supervisortrusts the supervisee to act independently, leavingspace for the supervisee to deploy emerging skills andtest growing clinical abilities. However, “hands-off”supervision is not the absence of supervision!In general, supervisees need more hands-onsupervision when tasks are new and increasing amountsof hands-off supervision as they progress and increasetheir skills, confidence and competence. Superviseesalso value an intermediate zone that allows themto shift back and forth between monitored (hands-on)and independent (hands-off) practice.• Seeing patients with supervisor• Discussing mistakes• Opportunities to discuss patient management“Hands-off” supervision• Identifying crucial supervision moments• Allowing room to develop independence• Feeling trusted• Providing opportunities for de-briefing and discussion.From a supervisor’s point of view, both hands-on andhands-off supervision are active processes, requiringthe exercise of judgment.To work out how much hands-on and hands-offsupervision your supervisee needs, it may be helpfulto ask yourself: How far along the trajectoryof development are they? When is it time to intervene?ExtractionYou find out that your superviseehas only done two extractions throughoutthe course of her training. Although shehas been deemed competent, she is notconfident at all. The two extractions shehad done were of mobile deciduous teethand now she is being confrontedwith having to extract a fully rootedbaby tooth on a six-year-old.How would you handle this situation,keeping in mind the principles ofhands-on/hands-off supervision?4 Iedema, R, Brownhill, S, Lancashire, W, Haines, M, Shaw, T, Street, J & Rubin, G (2008). Hands on, Hands off: A model of effective clinical supervisionthat recognises trainee’s need for support and independence, (Final Research Report for Institute of Medical Education and Training and Sax Institute),Centre for Health Communication, University of Technology, Sydney.FIRST EDITION<strong>HETI</strong> The Superguide85