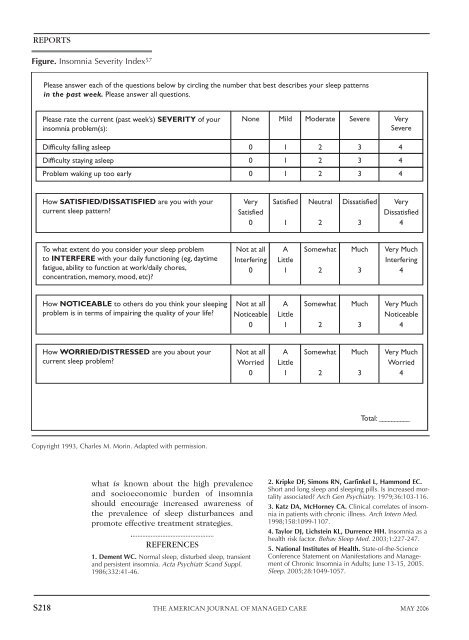
The Epidemiology and Diagnosis of Insomniaand nicotine dependence. The associationwith subsequent MDD was attenuated whenthe presence of other depressive symptomsat baseline was taken into account. 36However, a potential causative role forinsomnia in the development of MDD hasbeen postulated by several researchers. 40,41Whether insomnia is a precursor to MDD, anearly clinical hallmark of MDD, or the resultof etiological factors <strong>com</strong>mon to MDDremains to be clarified.Hohagen et al reported that severe andmoderate insomnia, but not mild insomnia,were associated with (unspecified) chronicsomatic disorders. In addition, when askedto rate their overall health status, patientswith severe insomnia rated their health as“moderate” (60%) or “bad” (25%) far morefrequently than those with no insomnia(41% and 4%, respectively). 38The same study also showed a strongcorrelation between insomnia severity andpsychiatric <strong>com</strong>orbidities. Among those withsevere insomnia, the prevalence of any psychiatricdisorder was 37.4% and the prevalenceof depression was 21.7%, <strong>com</strong>paredwith prevalence rates of 9.9% and 3.7%,respectively, for those reporting no sleepproblems. 38In addition to the strong correlationsbetween insomnia and psychiatric <strong>com</strong>orbidities,the prevalence of insomnia isincreased relative to healthy controls in thecontext of several chronic medical conditions,including osteoarthritis 42 ; rheumatoidarthritis 43 ; coronary artery disease 44,45 ; endstagerenal disease 46 ; type 1 and type 2 diabetesmellitus 47,48 ; and neurologic disorders,such as restless legs syndrome, 49 Parkinson’sdisease, 50 and Alzheimer’s disease. 51 Theseassociations and others are addressed indetail in the following article by Dr Ancoli-Israel (“The Impact and Prevalence ofChronic Insomnia and Other Sleep DisturbancesAssociated With Chronic Illness”).Clinical AssessmentAlthough more studies are necessary, evidenceindicates that (1) insomnia maycoexist with both psychological conditionsand physical illness, and (2) left untreated,it may be<strong>com</strong>e a long-term, chronic condition,particularly in women. Early interventionand management, therefore, could bebeneficial. However, the proportion ofinsomnia patients who report insomnia totheir physicians is quite small, and physiciansmay not adequately assess it. 36,52 Bothpatients and physicians may not recognizethe impact of poor sleep on daily functioningand the risk of serious accidents andpsychological sequelae. 5 Practice guidelinesdeveloped by the Standards of PracticeCommittee of the American Academy ofSleep Medicine strongly re<strong>com</strong>mend routineclinical screening for symptoms ofinsomnia during health examinations sothat treatment can be integrated into thepatient’s overall care. 53As with every illness, the cornerstone ofassessment for insomnia begins with a <strong>com</strong>prehensivehistory and screening for <strong>com</strong>orbidities,such as depressive and anxietydisorders, respiratory problems, and substanceuse, among others. 54 An in-depthsleep history is essential in identifying thecause of insomnia 5 and should includeresults of previous treatments. 54 Many of thetools that are useful in the assessment ofinsomnia are subjective questionnaires.Others include sleep logs, symptom checklists,psychological screening tests, andbed partner interviews. 5 The PittsburghSleep Quality Index is a sleep questionnairethat may provide useful informationabout sleep quality, timing, and duration. 55The Insomnia Severity Index (Figure) is areliable and valid instrument to quantifyperceived insomnia severity, includingnext-day consequences. 56 Nocturnal polysomnographyand daytime multiple sleeplatency testing are not re<strong>com</strong>mended for theroutine evaluation of insomnia unless othersleep disorders are suspected, such as sleeprelatedrespiratory disturbances or periodiclimb movement disorder.ConclusionMany questions remain unanswered inour understanding of insomnia. Futureresearch must clarify existing evidence surroundingthe exact nature of the relationshipbetween insomnia and psychologicaland physiologic <strong>com</strong>orbidities. In theabsence of <strong>com</strong>prehensive knowledge aboutthe active intricacies of the “resting” brain,VOL. 12, NO. 8, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S217
REPORTSFigure. Insomnia Severity Index 57Please answer each of the questions below by circling the number that best describes your sleep patternsin the past week. Please answer all questions.Please rate the current (past week’s) SEVERITY of yourinsomnia problem(s):None Mild Moderate Severe VerySevereDifficulty falling asleep01234Difficulty staying asleep01234Problem waking up too early01234How SATISFIED/DISSATISFIED are you with yourcurrent sleep pattern?VerySatisfied0Satisfied1Neutral2Dissatisfied3VeryDissatisfied4To what extent do you consider your sleep problemto INTERFERE with your daily functioning (eg, daytimefatigue, ability to function at work/daily chores,concentration, memory, mood, etc)?Not at allInterfering0ALittle1Somewhat2Much3Very MuchInterfering4How NOTICEABLE to others do you think your sleepingproblem is in terms of impairing the quality of your life?Not at allNoticeable0ALittle1Somewhat2Much3Very MuchNoticeable4How WORRIED/DISTRESSED are you about yourcurrent sleep problem?Not at allWorried0ALittle1Somewhat2Much3Very MuchWorried4Total: __________Copyright 1993, Charles M. Morin. Adapted with permission.what is known about the high prevalenceand socioeconomic burden of insomniashould encourage increased awareness ofthe prevalence of sleep disturbances andpromote effective treatment strategies.REFERENCES1. Dement WC. Normal sleep, disturbed sleep, transientand persistent insomnia. Acta Psychiatr Scand Suppl.1986;332:41-46.2. Kripke DF, Simons RN, Garfinkel L, Hammond EC.Short and long sleep and sleeping pills. Is increased mortalityassociated? Arch Gen Psychiatry. 1979;36:103-116.3. Katz DA, McHorney CA. Clinical correlates of insomniain patients with chronic illness. Arch Intern Med.1998;158:1099-1107.4. Taylor DJ, Lichstein KL, Durrence HH. Insomnia as ahealth risk factor. Behav Sleep Med. 2003;1:227-247.5. National Institutes of Health. State-of-the-ScienceConference Statement on Manifestations and Managementof Chronic Insomnia in Adults; June 13-15, 2005.Sleep. 2005;28:1049-1057.S218 THE AMERICAN JOURNAL OF MANAGED CARE MAY 2006
- Page 1 and 2:
Practice Management Tips ForSHIFT W
- Page 3 and 4:
Patient QuestionnaireDo you often f
- Page 5 and 6:
Sleep/Wake LogIn bedOut of bedLight
- Page 7 and 8:
PHQ-9 QUICK DEPRESSION ASSESSMENTFo
- Page 9 and 10:
Insomnia Severity IndexPlease answe
- Page 11 and 12:
Take-Away PointsSHIFT WORK DISORDER
- Page 13 and 14:
SHIFT WORKDISORDERBright Light Ther
- Page 40 and 41:
PrimarycareScreeningfor depressioni
- Page 42 and 43:
PrimarycareThescreening questionnai
- Page 44 and 45:
Shift-work disorderContents and Fac
- Page 46 and 47:
Shift-work disorderThe diagnosis of
- Page 48 and 49:
Shift-work disorderas heightened le
- Page 50 and 51: Shift-work disorderFigure 1 Risk ra
- Page 52 and 53: Shift-work disorderare not function
- Page 54 and 55: The characterization andpathology o
- Page 56 and 57: Shift-work disorderFigure 2 Sleep/w
- Page 58 and 59: Shift-work disorderFigure 3 Blood p
- Page 60 and 61: Recognition of shift-workdisorder i
- Page 62 and 63: Shift-work disorderThe timing of sh
- Page 64 and 65: Shift-work disorderthe other potent
- Page 66 and 67: Managing the patient withshift-work
- Page 68 and 69: Shift-work disorderFigure 3 Optimal
- Page 70 and 71: Shift-work disorderfor a motor vehi
- Page 72 and 73: Shift-work disordermoderate caffein
- Page 74 and 75: Supplement toAvailable at jfponline
- Page 76 and 77: Armodafinil for Treatment of Excess
- Page 78 and 79: Armodafinil for Treatment of Excess
- Page 80 and 81: Armodafinil for Treatment of Excess
- Page 82 and 83: Armodafinil for Treatment of Excess
- Page 84 and 85: Armodafinil for Treatment of Excess
- Page 86 and 87: Armodafinil for Treatment of Excess
- Page 88 and 89: Armodafinil for Treatment of Excess
- Page 90 and 91: Armodafinil for Treatment of Excess
- Page 92 and 93: Armodafinil for Treatment of Excess
- Page 94 and 95: Armodafinil for Treatment of Excess
- Page 96 and 97: Armodafinil for Treatment of Excess
- Page 98 and 99: The Epidemiology and Diagnosis of I
- Page 102 and 103: The Epidemiology and Diagnosis of I
- Page 120 and 121: CIRCADIAN RHYTHM SLEEP DISORDERSPra
- Page 122 and 123: Table 2— AASM Levels of Recommend
- Page 124 and 125: 3.2.1.1 Both the Morningness-Evenin
- Page 126 and 127: Five studies used one of the newer
- Page 128 and 129: as an indicator of phase in sighted
- Page 130 and 131: 4.4 Advanced Sleep Phase DisorderBe
- Page 132 and 133: 45. Walsh, JK, Randazzo, AC, Stone,
- Page 134: 123. Van Someren, EJ, Kessler, A, M
- Page 142 and 143: Table 1—Subject Demographicsn M:F
- Page 144 and 145: Scale. 28 The simple reaction time
- Page 146 and 147: Median RT (msec)1600A14001200100080
- Page 148 and 149: 10Mentally AExhaustedSharpScore8642
- Page 150 and 151:
Current Treatment Options in Neurol
- Page 152 and 153:
398 Sleep Disordersand sleep loss,
- Page 154 and 155:
400 Sleep DisordersTable 1. Treatme
- Page 156 and 157:
402 Sleep DisordersStandard dosageC
- Page 158 and 159:
404 Sleep DisordersStandard procedu
- Page 160 and 161:
406 Sleep DisordersCaffeineMelatoni
- Page 162 and 163:
408 Sleep DisordersWake-promoting a
- Page 164 and 165:
410 Sleep Disordersnight shift: ada