Recognition of shift-workdisorder in primary careJonathan R. L. Schwartz, MDUniversity of Oklahoma Health Sciences CenterINTEGRIS Sleep Disorders Center of OklahomaOklahoma City, OklahomaPractice re<strong>com</strong>mendationsy To recognize shift-work disorder (SWD),primary care physicians can screen forpersistent excessive sleepiness (ES)and insomnia in patients who worknight or rotating shifts (SOR: B).y If SWD is suspected, a differential diagnosisshould be generated, as ES and insomniaare <strong>com</strong>monly associated with othermorbidities. Ask patients about symptoms ofother <strong>com</strong>mon sleep/wake disorders, suchas obstructive sleep apnea and periodiclimb movement disorder (SOR: B).y The Epworth Sleepiness Scale is a usefultool for subjectively evaluating ES (SOR: A).Shift-work disorder (SWD) is experienced by individualswhose work schedule overlaps with the normalsleep period, causing misalignment between thebody’s endogenous circadian clock and the time at whichthe worker is able to rest. The International Classificationof Sleep Disorders, 2nd edition (ICSD-2) defines SWD as thepresence of excessive sleepiness (ES) and/or insomnia forat least 1 month, in association with a shift-work schedule. 1This classification results in the shift-work population beingseparated into 3 distinct groups: those who have no impairment;those who have impairment but do not meet theICSD-2 criteria for the diagnosis of SWD; and those who haveSWD. Individuals in the last 2 groups are less likely to be ableto meet the demands of shift work and, therefore, often returnto non–shift-work schedules or retire from the workforce. Thiscreates a “healthy worker effect,” whereby workers remainingon night- or rotating-shift patterns are the best suited for thistype of work. 2,3 However, retirement or changes to shift-workschedules are not an option for many workers, and patientswith SWD must be recognized and treated in order to preservetheir health and livelihood.This article aims to characterize the symptoms and riskfactors associated with SWD, with a view to assisting primarycare physicians in the diagnosis and recognition of this consistentlyunderrecognized sleep/wake disorder. 4Dr Schwartz reports that he serves as a consultant toand on the speakers bureaus of AstraZeneca, BoehringerIngelheim Pharmaceuticals, Inc., Cephalon, Inc., Pfizer Inc,Sepracor Inc., Takeda Pharmaceuticals North America, Inc,and GlaxoSmithKline.Symptoms of SWDInsomnia and ES (drowsiness and a propensity to sleep) arethe defining symptoms of SWD and can result in fatigue (wearinessand depleted energy), difficulty concentrating, reducedwork performance, headache, irritability or depressed mood,and feeling unrefreshed after sleeping. 4,5 The consequences ofinsomnia and ES may, therefore, also be useful warning signsfor SWD, and patients presenting with one or more of thesesequelae should be evaluated for risk factors for SWD andasked about their symptoms using the differential diagnosisdescribed below and in the Figure.S18 January 2010 / Vol 59, No 1 • Supplement to The Journal of Family Practice
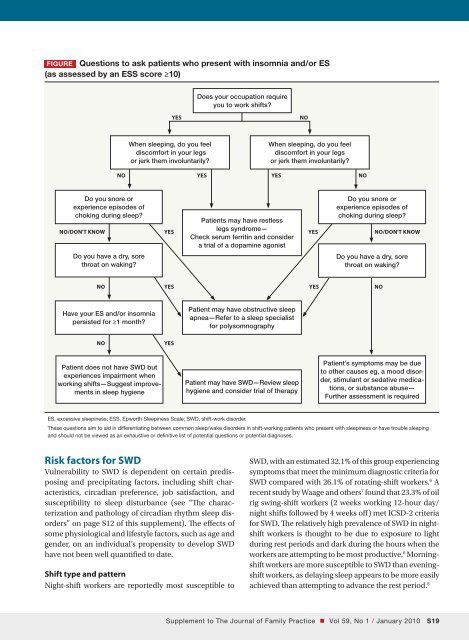
figure Questions to ask patients who present with insomnia and/or ES(as assessed by an ESS score ≥10)Does your occupation requireyou to work shifts?YESNoWhen sleeping, do you feeldis<strong>com</strong>fort in your legsor jerk them involuntarily?When sleeping, do you feeldis<strong>com</strong>fort in your legsor jerk them involuntarily?NoYesYesNoDo you snore orDo you snore orexperience episodes ofexperience episodes ofchoking during sleep?No/Don't know YesPatients may have restlesslegs syndrome—Check serum ferritin and considera trial of a dopamine agonistYeschoking during sleep?No/Don't knowDo you have a dry, sorethroat on waking?Do you have a dry, sorethroat on waking?No Yes Yes NoHave your ES and/or insomniapersisted for ≥1 month?Patient may have obstructive sleepapnea—Refer to a sleep specialistfor polysomnographyNoYesPatient does not have SWD butexperiences impairment whenworking shifts—Suggest improvementsin sleep hygienePatient may have SWD—Review sleephygiene and consider trial of therapyPatient’s symptoms may be dueto other causes eg, a mood disorder,stimulant or sedative medications,or substance abuse—Further assessment is requiredES, excessive sleepiness; ESS, Epworth Sleepiness Scale; SWD, shift-work disorder.These questions aim to aid in differentiating between <strong>com</strong>mon sleep/wake disorders in shift-working patients who present with sleepiness or have trouble sleepingand should not be viewed as an exhaustive or definitive list of potential questions or potential diagnoses.Risk factors for SWDVulnerability to SWD is dependent on certain predisposingand precipitating factors, including shift characteristics,circadian preference, job satisfaction, andsusceptibility to sleep disturbance (see “The characterizationand pathology of circadian rhythm sleep disorders”on page S12 of this supplement). The effects ofsome physiological and lifestyle factors, such as age andgender, on an individual’s propensity to develop SWDhave not been well quantified to date.Shift type and patternNight-shift workers are reportedly most susceptible toSWD, with an estimated 32.1% of this group experiencingsymptoms that meet the minimum diagnostic criteria forSWD <strong>com</strong>pared with 26.1% of rotating-shift workers. 6 Arecent study by Waage and others 7 found that 23.3% of oilrig swing-shift workers (2 weeks working 12-hour day/night shifts followed by 4 weeks off) met ICSD-2 criteriafor SWD. The relatively high prevalence of SWD in nightshiftworkers is thought to be due to exposure to lightduring rest periods and dark during the hours when theworkers are attempting to be most productive. 6 Morningshiftworkers are more susceptible to SWD than eveningshiftworkers, as delaying sleep appears to be more easilyachieved than attempting to advance the rest period. 8Supplement to The Journal of Family Practice • Vol 59, No 1 / January 2010 S19
- Page 1 and 2:
Practice Management Tips ForSHIFT W
- Page 3 and 4:
Patient QuestionnaireDo you often f
- Page 5 and 6:
Sleep/Wake LogIn bedOut of bedLight
- Page 7 and 8:
PHQ-9 QUICK DEPRESSION ASSESSMENTFo
- Page 9 and 10: Insomnia Severity IndexPlease answe
- Page 11 and 12: Take-Away PointsSHIFT WORK DISORDER
- Page 13 and 14: SHIFT WORKDISORDERBright Light Ther
- Page 40 and 41: PrimarycareScreeningfor depressioni
- Page 42 and 43: PrimarycareThescreening questionnai
- Page 44 and 45: Shift-work disorderContents and Fac
- Page 46 and 47: Shift-work disorderThe diagnosis of
- Page 48 and 49: Shift-work disorderas heightened le
- Page 50 and 51: Shift-work disorderFigure 1 Risk ra
- Page 52 and 53: Shift-work disorderare not function
- Page 54 and 55: The characterization andpathology o
- Page 56 and 57: Shift-work disorderFigure 2 Sleep/w
- Page 58 and 59: Shift-work disorderFigure 3 Blood p
- Page 62 and 63: Shift-work disorderThe timing of sh
- Page 64 and 65: Shift-work disorderthe other potent
- Page 66 and 67: Managing the patient withshift-work
- Page 68 and 69: Shift-work disorderFigure 3 Optimal
- Page 70 and 71: Shift-work disorderfor a motor vehi
- Page 72 and 73: Shift-work disordermoderate caffein
- Page 74 and 75: Supplement toAvailable at jfponline
- Page 76 and 77: Armodafinil for Treatment of Excess
- Page 78 and 79: Armodafinil for Treatment of Excess
- Page 80 and 81: Armodafinil for Treatment of Excess
- Page 82 and 83: Armodafinil for Treatment of Excess
- Page 84 and 85: Armodafinil for Treatment of Excess
- Page 86 and 87: Armodafinil for Treatment of Excess
- Page 88 and 89: Armodafinil for Treatment of Excess
- Page 90 and 91: Armodafinil for Treatment of Excess
- Page 92 and 93: Armodafinil for Treatment of Excess
- Page 94 and 95: Armodafinil for Treatment of Excess
- Page 96 and 97: Armodafinil for Treatment of Excess
- Page 98 and 99: The Epidemiology and Diagnosis of I
- Page 100 and 101: The Epidemiology and Diagnosis of I
- Page 102 and 103: The Epidemiology and Diagnosis of I
- Page 120 and 121:
CIRCADIAN RHYTHM SLEEP DISORDERSPra
- Page 122 and 123:
Table 2— AASM Levels of Recommend
- Page 124 and 125:
3.2.1.1 Both the Morningness-Evenin
- Page 126 and 127:
Five studies used one of the newer
- Page 128 and 129:
as an indicator of phase in sighted
- Page 130 and 131:
4.4 Advanced Sleep Phase DisorderBe
- Page 132 and 133:
45. Walsh, JK, Randazzo, AC, Stone,
- Page 134:
123. Van Someren, EJ, Kessler, A, M
- Page 142 and 143:
Table 1—Subject Demographicsn M:F
- Page 144 and 145:
Scale. 28 The simple reaction time
- Page 146 and 147:
Median RT (msec)1600A14001200100080
- Page 148 and 149:
10Mentally AExhaustedSharpScore8642
- Page 150 and 151:
Current Treatment Options in Neurol
- Page 152 and 153:
398 Sleep Disordersand sleep loss,
- Page 154 and 155:
400 Sleep DisordersTable 1. Treatme
- Page 156 and 157:
402 Sleep DisordersStandard dosageC
- Page 158 and 159:
404 Sleep DisordersStandard procedu
- Page 160 and 161:
406 Sleep DisordersCaffeineMelatoni
- Page 162 and 163:
408 Sleep DisordersWake-promoting a
- Page 164 and 165:
410 Sleep Disordersnight shift: ada