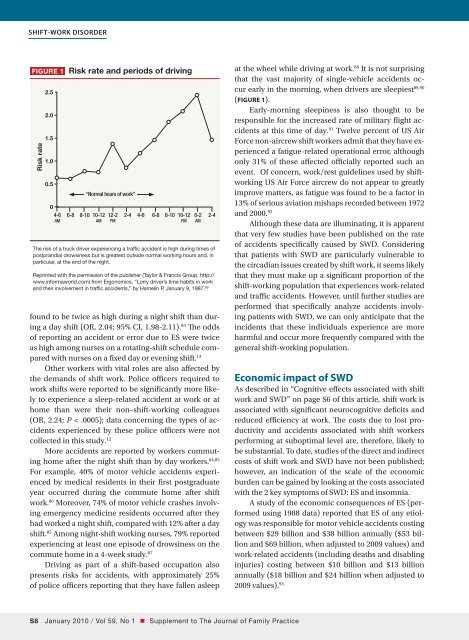
Shift-work disorderFigure 1 Risk rate and periods of drivingRisk rate2.52.01.51.00.5“Normal hours of work”04-6 6-8 8-10 10-12 12-2 2-4 4-6 6-8 8-10 10-12 0-2 2-4am am pm pm amThe risk of a truck driver experiencing a traffic accident is high during times ofpostprandial drowsiness but is greatest outside normal working hours and, inparticular, at the end of the night.Reprinted with the permission of the publisher (Taylor & Francis Group, http://www.informaworld.<strong>com</strong>) from Ergonomics. “Lorry driver’s time habits in workand their involvement in traffic accidents,” by Hamelin P, January 9, 1987. 89found to be twice as high during a night shift than duringa day shift (OR, 2.04; 95% CI, 1.98-2.11). 83 The oddsof reporting an accident or error due to ES were twiceas high among nurses on a rotating-shift schedule <strong>com</strong>paredwith nurses on a fixed day or evening shift. 13Other workers with vital roles are also affected bythe demands of shift work. Police officers required towork shifts were reported to be significantly more likelyto experience a sleep-related accident at work or athome than were their non–shift-working colleagues(OR, 2.24; P < .0005); data concerning the types of accidentsexperienced by these police officers were notcollected in this study. 12More accidents are reported by workers <strong>com</strong>mutinghome after the night shift than by day workers. 84,85For example, 40% of motor vehicle accidents experiencedby medical residents in their first postgraduateyear occurred during the <strong>com</strong>mute home after shiftwork. 86 Moreover, 74% of motor vehicle crashes involvingemergency medicine residents occurred after theyhad worked a night shift, <strong>com</strong>pared with 12% after a dayshift. 85 Among night-shift working nurses, 79% reportedexperiencing at least one episode of drowsiness on the<strong>com</strong>mute home in a 4-week study. 87Driving as part of a shift-based occupation alsopresents risks for accidents, with approximately 25%of police officers reporting that they have fallen asleepat the wheel while driving at work. 88 It is not surprisingthat the vast majority of single-vehicle accidents occurearly in the morning, when drivers are sleepiest 89,90(FIGURE 1).Early-morning sleepiness is also thought to beresponsible for the increased rate of military flight accidentsat this time of day. 91 Twelve percent of US AirForce non-aircrew shift workers admit that they have experienceda fatigue-related operational error, althoughonly 31% of those affected officially reported such anevent. Of concern, work/rest guidelines used by shiftworkingUS Air Force aircrew do not appear to greatlyimprove matters, as fatigue was found to be a factor in13% of serious aviation mishaps recorded between 1972and 2000. 92Although these data are illuminating, it is apparentthat very few studies have been published on the rateof accidents specifically caused by SWD. Consideringthat patients with SWD are particularly vulnerable tothe circadian issues created by shift work, it seems likelythat they must make up a significant proportion of theshift-working population that experiences work-relatedand traffic accidents. However, until further studies areperformed that specifically analyze accidents involvingpatients with SWD, we can only anticipate that theincidents that these individuals experience are moreharmful and occur more frequently <strong>com</strong>pared with thegeneral shift-working population.Economic impact of SWDAs described in “Cognitive effects associated with shiftwork and SWD” on page S6 of this article, shift work isassociated with significant neurocognitive deficits andreduced efficiency at work. The costs due to lost productivityand accidents associated with shift workersperforming at suboptimal level are, therefore, likely tobe substantial. To date, studies of the direct and indirectcosts of shift work and SWD have not been published;however, an indication of the scale of the economicburden can be gained by looking at the costs associatedwith the 2 key symptoms of SWD: ES and insomnia.A study of the economic consequences of ES (performedusing 1988 data) reported that ES of any etiologywas responsible for motor vehicle accidents costingbetween $29 billion and $38 billion annually ($53 billionand $69 billion, when adjusted to 2009 values) andwork-related accidents (including deaths and disablinginjuries) costing between $10 billion and $13 billionannually ($18 billion and $24 billion when adjusted to2009 values). 93S January 2010 / Vol 59, No 1 • Supplement to The Journal of Family Practice
Figure 2 Shift-related factors likely to affect attrition in the emergency medical professionsRisk of accidents ofself-harm at work, eg,percutaneous injuryInsomniaIncreased risk of <strong>com</strong>orbidities,eg, GI disorders, CVD,depression, and cancerRisk of traffic accidents,particularly during the <strong>com</strong>mutehome from workShift-related factorsleading to high rates ofattrition in the medicalprofessionsOn-call stressExcessive sleepinessSleep deprivationReductions in socialinteractions, particularly timewith the familyCVD, cardiovascular disease; GI, gastrointestinal.Studies of patients with insomnia of unspecifiedetiology reveal the extent of the cost burden of thissymptom. An observational US study found that average6-month total costs (ie, direct and indirect costs) wereapproximately $1253 higher for an adult (age 18–64years) with insomnia than for a matched control withoutinsomnia. 94A recently reported Canadian study highlighted thelarge contribution of indirect costs to the total costs associatedwith insomnia. 95 Direct costs included thosefor doctors’ visits, transportation to the visits, and prescriptionand over-the-counter drugs. Indirect costs associatedwith insomnia included those for lost productivityand job absenteeism; these accounted for 91% ofall costs. On average, the total annual costs incurred by apatient with insomnia syndrome (defined as those whoused a sleep-promoting agent ≥3 nights per week and/or were dissatisfied with sleep, had insomnia symptoms≥3 nights per week for ≥1 month, and experiencedpsychological distress or daytime impairment) 95 wereC$5010 (C$293 direct and C$4717 indirect). For a patientwith insomnia symptoms, average annual totalcosts were calculated to be C$1431 (C$160 direct andC$1271 indirect). By <strong>com</strong>parison, a good sleeper (ie, astudy subject who reported being happy with his or hersleep, did not report symptoms of insomnia, and did notuse sleep-promoting medication) was found to incuraverage annual costs of C$421. 95More detailed assessment is required of the costsincurred specifically in patients with SWD, but there isclearly an economic rationale for early diagnosis andtreatment of the symptoms of SWD.SummaryWhat is clear from this review is that, while informationon shift work is relatively abundant, data concerningSWD are meager. For example, epidemiologic data onSWD are sparse, in part because many investigators instudies of shift workers do not take the seemingly logicalstep of assessing SWD in their subjects. However, differentiatingbetween shift workers who experience transientsymptoms associated with adapting to a new shiftschedule and individuals with SWD is <strong>com</strong>plex and maylead to underrecognition of this condition. Similarly,there are few data on the <strong>com</strong>orbidities experienced byindividuals diagnosed with SWD and further studies arewarranted. The increased risk of illness demonstratedby shift-working individuals may be even greater in patientswith SWD due to their intrinsic—and poorly understood—vulnerabilityto the effects of shift work.The studies described here show that the burden ofSWD is multifactorial, and it includes impairment of patients’relationships and health and reduces their efficiencyat work. 6 Again, there are very few data on the economicburden of SWD, although reduced productivity and thecost of accidents in the workplace and while driving arelikely to be high. Additional research is needed in this area.Shift workers, including public service workers, mustmake difficult decisions during times of day when theySupplement to The Journal of Family Practice • Vol 59, No 1 / January 2010 S
- Page 1 and 2: Practice Management Tips ForSHIFT W
- Page 3 and 4: Patient QuestionnaireDo you often f
- Page 5 and 6: Sleep/Wake LogIn bedOut of bedLight
- Page 7 and 8: PHQ-9 QUICK DEPRESSION ASSESSMENTFo
- Page 9 and 10: Insomnia Severity IndexPlease answe
- Page 11 and 12: Take-Away PointsSHIFT WORK DISORDER
- Page 13 and 14: SHIFT WORKDISORDERBright Light Ther
- Page 40 and 41: PrimarycareScreeningfor depressioni
- Page 42 and 43: PrimarycareThescreening questionnai
- Page 44 and 45: Shift-work disorderContents and Fac
- Page 46 and 47: Shift-work disorderThe diagnosis of
- Page 48 and 49: Shift-work disorderas heightened le
- Page 52 and 53: Shift-work disorderare not function
- Page 54 and 55: The characterization andpathology o
- Page 56 and 57: Shift-work disorderFigure 2 Sleep/w
- Page 58 and 59: Shift-work disorderFigure 3 Blood p
- Page 60 and 61: Recognition of shift-workdisorder i
- Page 62 and 63: Shift-work disorderThe timing of sh
- Page 64 and 65: Shift-work disorderthe other potent
- Page 66 and 67: Managing the patient withshift-work
- Page 68 and 69: Shift-work disorderFigure 3 Optimal
- Page 70 and 71: Shift-work disorderfor a motor vehi
- Page 72 and 73: Shift-work disordermoderate caffein
- Page 74 and 75: Supplement toAvailable at jfponline
- Page 76 and 77: Armodafinil for Treatment of Excess
- Page 78 and 79: Armodafinil for Treatment of Excess
- Page 80 and 81: Armodafinil for Treatment of Excess
- Page 82 and 83: Armodafinil for Treatment of Excess
- Page 84 and 85: Armodafinil for Treatment of Excess
- Page 86 and 87: Armodafinil for Treatment of Excess
- Page 88 and 89: Armodafinil for Treatment of Excess
- Page 90 and 91: Armodafinil for Treatment of Excess
- Page 92 and 93: Armodafinil for Treatment of Excess
- Page 94 and 95: Armodafinil for Treatment of Excess
- Page 96 and 97: Armodafinil for Treatment of Excess
- Page 98 and 99: The Epidemiology and Diagnosis of I
- Page 100 and 101:
The Epidemiology and Diagnosis of I
- Page 102 and 103:
The Epidemiology and Diagnosis of I
- Page 120 and 121:
CIRCADIAN RHYTHM SLEEP DISORDERSPra
- Page 122 and 123:
Table 2— AASM Levels of Recommend
- Page 124 and 125:
3.2.1.1 Both the Morningness-Evenin
- Page 126 and 127:
Five studies used one of the newer
- Page 128 and 129:
as an indicator of phase in sighted
- Page 130 and 131:
4.4 Advanced Sleep Phase DisorderBe
- Page 132 and 133:
45. Walsh, JK, Randazzo, AC, Stone,
- Page 134:
123. Van Someren, EJ, Kessler, A, M
- Page 142 and 143:
Table 1—Subject Demographicsn M:F
- Page 144 and 145:
Scale. 28 The simple reaction time
- Page 146 and 147:
Median RT (msec)1600A14001200100080
- Page 148 and 149:
10Mentally AExhaustedSharpScore8642
- Page 150 and 151:
Current Treatment Options in Neurol
- Page 152 and 153:
398 Sleep Disordersand sleep loss,
- Page 154 and 155:
400 Sleep DisordersTable 1. Treatme
- Page 156 and 157:
402 Sleep DisordersStandard dosageC
- Page 158 and 159:
404 Sleep DisordersStandard procedu
- Page 160 and 161:
406 Sleep DisordersCaffeineMelatoni
- Page 162 and 163:
408 Sleep DisordersWake-promoting a
- Page 164 and 165:
410 Sleep Disordersnight shift: ada