HHC Health & Home Care Clinical Policy And
HHC Health & Home Care Clinical Policy And
HHC Health & Home Care Clinical Policy And

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>HHC</strong> HEALTH & HOME CARE Section: 11-7<br />
Pediatrics: Tracheostomy Suctioning __RN<br />
PURPOSE:<br />
To clear the airway and remove secretions which cannot<br />
effectively be coughed up.<br />
CONSIDERATIONS:<br />
1. The cardinal indication for suctioning is the<br />
presence of coarse breath sounds or rhonchi that<br />
persist in spite of the patient's effort to cough. Other<br />
indications include constant cough, retractions and<br />
inability to clear secretions.<br />
2. Suctioning should only be done as needed to keep<br />
the tracheostomy tube patent. Need can be<br />
determined by chest auscultation and signs of<br />
increased respiratory effort.<br />
3. Cardiac arrhythmia, vagal stimulation, and<br />
laryngospasm may occur during suctioning. In the<br />
event of heart irregularity or color changes,<br />
suctioning should be discontinued.<br />
4. Oxygen depletion may occur. Therefore, preoxygenate<br />
before and after the procedure, unless<br />
directed otherwise by the physician.<br />
5. Suction apparatus should be cleaned or tubing<br />
changed according to durable medical equipment<br />
(DME) vendor's protocol.<br />
6. Suction apparatus should be set at 40-60mm Hg -<br />
neonate to six months, 60-100mm Hg - six months<br />
to 10 years, 80-120mm Hg - 10 years to adolescent.<br />
7. Occlusion of the tracheostomy tube is life threatening.<br />
Infants and children are at greater risk than adults<br />
because of the smaller diameter of the tube.<br />
8. To avoid trauma to the tracheobronchial wall, the<br />
suction catheter should be marked prior to<br />
suctioning. Calibrated catheters may be utilized or<br />
measurement may be performed by placing suction<br />
catheter through sample tracheostomy tube (same<br />
size as child's). Mark a line on the catheter, which<br />
will provide a guide to inserting catheter. Suction<br />
catheter should be inserted to a point just shortly<br />
beyond the end of tracheostomy tube.<br />
9. In children who require long-term cannulation with a<br />
tracheostomy tube and who are not<br />
immunosuppressed, using a sterile suction catheter for<br />
each suction pass may not be optimal. Replacing the<br />
suction catheter at least every 24 hours and using a<br />
clean, no-touch technique may be used.<br />
10. If the clean, no-touch is an option, the<br />
recommendation of the equipment company<br />
supplying the tracheostomy supplies should be<br />
followed to clean and store the suction catheter<br />
between suctioning.<br />
11. Avoid suctioning after meals.<br />
EQUIPMENT:<br />
Suction apparatus capable of producing negative<br />
pressure (standard is 80mm of pressure, range is<br />
from 40-100)<br />
Container for secretions<br />
Suction catheter (the diameter should be approximately<br />
half the diameter of the tracheostomy tube) No. 8-10<br />
Two cups<br />
Sterile saline<br />
Sterile water<br />
Impervious trash bag<br />
Gloves<br />
Supplemental oxygen<br />
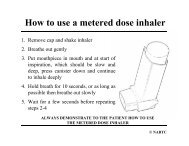
PROCEDURE:<br />
1. Adhere to Universal Precautions.<br />
2. Explain procedure to caregiver and patient, in age<br />
appropriate manner.<br />
3. Test suction apparatus.<br />
4. Check tracheostomy tube to be sure it is tied<br />
securely.<br />
5. Remove sterile catheter from wrapping and attach<br />
to plastic suction tubing.<br />
6. Aspirate secretions.<br />
a. Leaving thumb off air vent, gently insert<br />
catheter into tracheostomy to premeasured line.<br />
b. Gently aspirate secretions by covering the air<br />
vent and rotating catheter. Never exceed 3 to 4<br />
seconds with each suctioning.<br />
c. In presence of tenacious secretions, 0.5cc to<br />
2cc of sterile saline may be instilled into<br />
tracheostomy tube prior to suctioning.<br />
d. Each time you remove the catheter, allow the<br />
patient three to five breaths before repeating<br />
procedure or re-oxygenate with supplemental<br />
oxygen.<br />
e. The oral cavity can be suctioned after the<br />
tracheostomy tube is cleared. Never suction<br />
oral cavity first unless catheter is changed<br />
before inserting into tracheostomy tube.<br />
f. Rinse catheter tubing with sterile water to<br />
prevent clogging.<br />
g. Auscultate lungs to ascertain results.<br />
7. Discard soiled supplies and solutions in appropriate<br />
containers.<br />
AFTER CARE:<br />
1. Reassure patient and caregiver.<br />
2. Document in patient's record:<br />
a. Color of patient.<br />
b. Consistency, color and amount of secretions.<br />
c. Patient's tolerance of procedure.<br />
d. Changes in vital signs or complications that<br />
may have occurred.<br />
e. Instructions given to caregiver.<br />
3. Clean and change tubing according to DME<br />
supplier's guidelines.<br />
255