2017 HCHB_digital

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
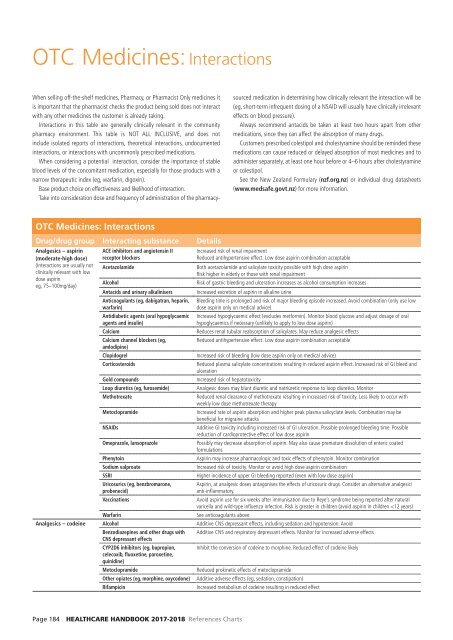
OTC Medicines: Interactions<br />
When selling off-the-shelf medicines, Pharmacy, or Pharmacist Only medicines it<br />
is important that the pharmacist checks the product being sold does not interact<br />
with any other medicines the customer is already taking.<br />
Interactions in this table are generally clinically relevant in the community<br />
pharmacy environment. This table is NOT ALL INCLUSIVE, and does not<br />
include isolated reports of interactions, theoretical interactions, undocumented<br />
interactions, or interactions with uncommonly prescribed medications.<br />
When considering a potential interaction, consider the importance of stable<br />
blood levels of the concomitant medication, especially for those products with a<br />
narrow therapeutic index (eg, warfarin, digoxin).<br />
Base product choice on effectiveness and likelihood of interaction.<br />
Take into consideration dose and frequency of administration of the pharmacy-<br />
sourced medication in determining how clinically relevant the interaction will be<br />
(eg, short-term infrequent dosing of a NSAID will usually have clinically irrelevant<br />
effects on blood pressure).<br />
Always recommend antacids be taken at least two hours apart from other<br />
medications, since they can affect the absorption of many drugs.<br />
Customers prescribed colestipol and cholestyramine should be reminded these<br />
medications can cause reduced or delayed absorption of most medicines and to<br />
administer separately, at least one hour before or 4–6 hours after cholestyramine<br />
or colestipol.<br />
See the New Zealand Formulary (nzf.org.nz) or individual drug datasheets<br />
(www.medsafe.govt.nz) for more information.<br />
OTC Medicines: Interactions<br />
Drug/drug group Interacting substance Details<br />
Analgesics – aspirin<br />
(moderate-high dose)<br />
(Interactions are usually not<br />
clinically relevant with low<br />
dose aspirin<br />
eg, 75–100mg/day)<br />
ACE inhibitors and angiotensin II<br />
receptor blockers<br />
Acetazolamide<br />
Increased risk of renal impairment<br />
Reduced antihypertensive effect. Low dose aspirin combination acceptable<br />
Both acetazolamide and salicylate toxicity possible with high dose aspirin<br />
Risk higher in elderly or those with renal impairment<br />
Risk of gastric bleeding and ulceration increases as alcohol consumption increases<br />
Increased excretion of aspirin in alkaline urine<br />
Bleeding time is prolonged and risk of major bleeding episode increased. Avoid combination (only use low<br />
dose aspirin only on medical advice)<br />
Increased hypoglycaemic effect (excludes metformin). Monitor blood glucose and adjust dosage of oral<br />
hypoglycaemics if necessary (unlikely to apply to low dose aspirin)<br />
Reduces renal tubular reabsorption of salicylates. May reduce analgesic effects<br />
Reduced antihypertensive effect. Low dose aspirin combination acceptable<br />
Alcohol<br />
Antacids and urinary alkalinisers<br />
Anticoagulants (eg, dabigatran, heparin,<br />
warfarin)<br />
Antidiabetic agents (oral hypoglycaemic<br />
agents and insulin)<br />
Calcium<br />
Calcium channel blockers (eg,<br />
amlodipine)<br />
Clopidogrel<br />
Increased risk of bleeding (low dose aspirin only on medical advice)<br />
Corticosteroids<br />
Reduced plasma salicylate concentrations resulting in reduced aspirin effect. Increased risk of GI bleed and<br />
ulceration<br />
Gold compounds<br />
Increased risk of hepatotoxicity<br />
Loop diuretics (eg, furosemide) Analgesic doses may blunt diuretic and natriuretic response to loop diuretics. Monitor<br />
Methotrexate<br />
Reduced renal clearance of methotrexate resulting in increased risk of toxicity. Less likely to occur with<br />
weekly low dose methotrexate therapy<br />
Metoclopramide<br />
Increased rate of aspirin absorption and higher peak plasma salicyclate levels. Combination may be<br />
beneficial for migraine attacks<br />
NSAIDs<br />
Additive GI toxicity including increased risk of GI ulceration. Possible prolonged bleeding time. Possible<br />
reduction of cardioprotective effect of low dose aspirin<br />
Omeprazole, lansoprazole<br />
Possibly may decrease absorption of aspirin. May also cause premature dissolution of enteric coated<br />
formulations<br />
Phenytoin<br />
Aspirin may increase pharmacologic and toxic effects of phenytoin. Monitor combination<br />
Sodium valproate<br />
Increased risk of toxicity. Monitor or avoid high dose aspirin combination<br />
SSRI<br />
Higher incidence of upper GI bleeding reported (even with low dose aspirin)<br />
Uricosurics (eg, benzbromarone, Aspirin, at analgesic doses antagonises the effects of uricosuric drugs. Consider an alternative analgesic/<br />
probenecid)<br />
anti-inflammatory.<br />
Vaccinations<br />
Avoid aspirin use for six weeks after immunisation due to Reye’s syndrome being reported after natural<br />
varicella and wild-type influenza infection. Risk is greater in children (avoid aspirin in children